Module 24: Acrolentiginous Melanoma
Source: Dermoscopy Educational Course Authors: Ralph P. Braun, Susana Puig, and Josep Malvehy
1. Learning Objectives
After completing this module, the learner should be able to:
- Describe the unique microanatomy of volar (palms and soles) skin, including the relationship between furrows (sulcus superficialis), ridges (crista superficialis), crista limitans, and crista intermedia, and explain how this anatomy determines dermoscopic pigment distribution in nevi versus melanoma.
- Identify the parallel ridge pattern (PRP) as the hallmark dermoscopic finding of early acrolentiginous melanoma (ALM), and recall its sensitivity (86%), specificity (99%), and positive predictive value (84%).
- Recognize the full spectrum of malignant dermoscopic patterns on volar skin: parallel ridge pattern, diffuse pigmentation with variable shades of brown, serrated pattern, atypical fibrillar pattern, milky-red pattern, and multicomponent pattern.
- Differentiate benign acral dermoscopic patterns (parallel furrow, lattice-like, fibrillar, globular, homogeneous, acral reticular) from malignant patterns, and explain why focal benign patterns within a lesion do not exclude melanoma.
- Apply the BRAAFF algorithm to systematically evaluate volar lesions, including correct scoring of positive criteria (irregular Blotch, parallel Ridge pattern, Asymmetry of structures, Asymmetry of colors) and negative criteria (parallel Furrow pattern, Fibrillar pattern).
- List conditions that can mimic the parallel ridge pattern (ethnic pigmentation, Laugier-Hunziker syndrome, Peutz-Jeghers syndrome, subcorneal hemorrhage, chemotherapy-induced pigmentation, congenital nevi) and describe distinguishing features for each.
- Explain the significance of lesion diameter in the evaluation of acquired melanocytic lesions on volar skin, specifically the 7 mm threshold.
- Recognize amelanotic and advanced ALM presentations, including the role of atypical vessels (corkscrew pattern), ulceration, hyperkeratosis, and remnant pigmentation as diagnostic clues.
2. Prerequisites
- Module 01: Introduction and Principles of Dermoscopy -- Equipment operation, polarized vs. nonpolarized dermoscopy, and image acquisition techniques.
- Module 02: Histopathologic Correlations of Dermoscopic Structures -- Understanding how melanin depth, chromophores, and histologic features produce dermoscopic colors and patterns.
- Module 03: Pattern Analysis Revised -- Geometric terminology, the concept of parallel lines on ridges as Clue #9 to malignancy, and the "Chaos and Clues" triage framework.
- Module 31: Palms and Soles (co-requisite or prerequisite) -- Detailed anatomy of volar skin, benign acral dermoscopic patterns (parallel furrow, lattice-like, fibrillar, globular, homogeneous, acral reticular), and the histologic basis for pigment distribution in acral nevi. Chapter 11b provides the foundational anatomy and benign patterns referenced throughout this module.
3. Key Concepts
Acrolentiginous Melanoma on Acral Skin
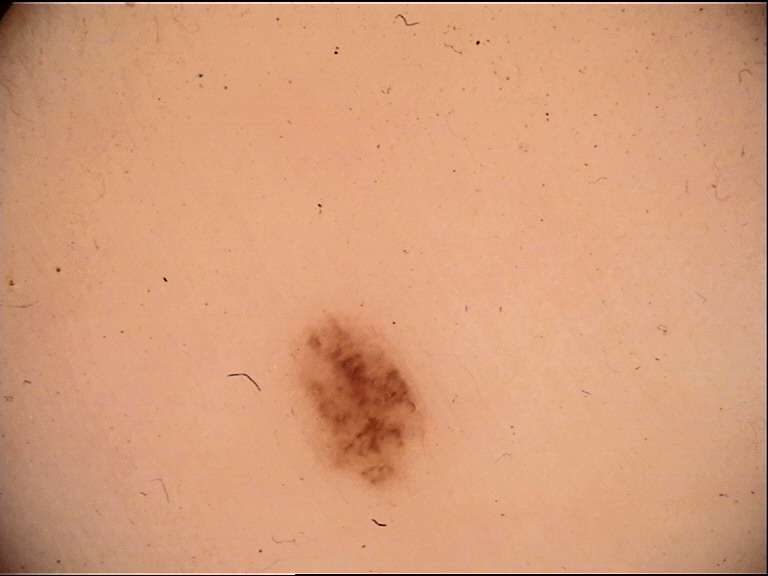
Acrolentiginous melanoma (ALM) is the melanoma subtype that arises on the glabrous (hairless, non-sun-exposed) skin of the palms, soles, and subungual regions. Although ALM is the least common melanoma subtype overall, it represents a disproportionately high percentage of melanomas in patients with darker skin phototypes (Fitzpatrick types IV-VI) and in Asian populations. The plantar surface (sole of the foot) is the most common site.
Parallel Pattern Analysis: The Central Paradigm
The fundamental principle of acral dermoscopy rests on a single anatomic observation:
- In acral nevi, melanocytes reside at the crista limitans, which corresponds to the skin furrows (sulcus superficialis). Melanin is transferred preferentially to keratinocytes in the furrows, producing the parallel furrow pattern (benign).
- In acral melanoma, malignant melanocytes proliferate around the crista intermedia, likely because melanocytic stem cells reside in this environment. The result is pigmentation located on the ridges (crista superficialis), producing the parallel ridge pattern (malignant).
This ridge-versus-furrow distinction is the single most important concept in acral dermoscopy and forms the basis of all acral dermoscopic algorithms.
Eccrine Duct Landmark
The openings of eccrine sweat glands are located on the ridges. On dermoscopy, these appear as regularly spaced whitish dots within pigmented bands. Their position helps the observer confirm whether pigmentation is on the ridges (malignant pattern) or in the furrows (benign pattern).
4. Core Content
4.1 Introduction and Anatomy

The skin on palms and soles has a unique anatomy due to the presence of alternating furrows and ridges, which creates the individualized dermatoglyphic patterns (fingerprints). Understanding the particular histologic anatomy of palms and soles is essential for correctly interpreting the significance of dermoscopic colors, structures, and patterns of lesions in these locations.
Key Anatomic Structures
| Structure | Location | Clinical Significance |
|---|---|---|
| Sulcus superficialis (furrow) | Surface depression between ridges | Corresponds to crista limitans; site of pigment deposition in nevi |
| Crista superficialis (ridge) | Elevated surface marking | Site of eccrine duct openings; site of pigment deposition in melanoma |
| Crista limitans | Deep dermal ridge beneath the furrow | Nevomelanocytic nests preferentially transfer melanin here |
| Crista intermedia | Deep dermal ridge beneath the surface ridge | Melanocytic stem cell niche; favored by malignant melanocytes |
| Eccrine ducts | Open on the ridges | Appear as whitish dots; landmark for identifying ridges |
In melanocytic nevi, nevomelanocytic nests may be found at the tips of rete ridges associated with both the crista intermedia and crista limitans; however, melanin is preferentially transferred to keratinocytes from nests at the crista limitans, resulting in the parallel furrow pattern. In early melanoma, malignant melanocytes favor growth in the environment surrounding the crista intermedia (potentially because melanocytic stem cells reside there), resulting in pigmentation on the ridges.
The dermoscopic patterns of benign lesions on volar skin are described in detail in Module 31 (Chapter 11b).
4.2 Malignant Dermoscopic Patterns on Volar (Glabrous) Skin
Six malignant patterns have been described for melanocytic lesions on volar skin:
4.2.1 Parallel Ridge Pattern (PRP)
The parallel ridge pattern is the most common and most specific dermoscopic finding in early (including in situ) acrolentiginous melanoma. It consists of linear pigmentation located predominantly on the ridges.
Diagnostic performance:
- Specificity: 99%
- Sensitivity: 86%
- Positive predictive value: 84%
Key characteristics:
- Band-like pigmentation on the surface ridges of the skin markings
- Whitish dots (eccrine duct openings) regularly distributed within the pigmented bands confirm ridge localization
- Typically found in the macular (flat) portions of volar melanomas
- Present in both in situ and invasive melanomas
In situ vs. invasive distinction:
- Melanoma in situ: Usually displays only tan to brown lines on the ridges without other colors or visible structures
- Invasive melanoma: May display pigmentation on the ridges, but it will rarely be the only feature seen and will rarely manifest as only tan to brown ridges; additional features such as blue-gray color, irregular dots, blue-white veil, and vascular structures are commonly present
Important exceptions -- conditions that can mimic the PRP:
- Ethnic pigmentation (darker skin phototypes) -- benign volar lesions may display a parallel ridge pattern
- Peutz-Jeghers syndrome -- mucocutaneous pigmentation syndrome
- Laugier-Hunziker syndrome -- benign acquired mucocutaneous hyperpigmentation; recognized by the clinical presentation of multiple small brownish macules on multiple fingers and lips
- Chemotherapy-induced volar pigmentation -- drug-related hyperpigmentation
- Exogenous dye -- external pigment application
- Subcorneal blood (hemorrhage) -- blood tracks along the least resistant tissue planes (possibly along eccrine glands), accumulating on the ridges and creating a parallel ridge pattern or "pebbles on the ridges" pattern. Subcorneal blood has a reddish-black color composed of droplets with smooth margins. The scraping test (paring down the stratum corneum with a scalpel) can confirm subcorneal hemorrhage by removing the blood and revealing normal underlying skin
- Congenital nevi -- can occasionally display a ridge pattern
4.2.2 Diffuse Pigmentation with Variable Shades of Brown and Serrated Pattern
The diffuse pigmentation with variable shades of brown is the second most common pattern seen in ALM. It consists of structureless diffuse pigmentation involving both the ridges and furrows, displaying various shades of brown color. This pattern can be seen in both in situ and invasive ALMs.
The serrated pattern is another feature occasionally encountered in ALM. It consists of projections (similar to streaks) at the edge of the tumor, producing a serrated or jagged peripheral margin.
4.2.3 Atypical Fibrillar Pattern
The fibrillar pattern on volar skin results from mechanical frictional forces (described in detail in Module 31, Chapter 11b). The distinction between benign and atypical (malignant) fibrillar patterns is critical:
Location considerations:
- Any lesion on the palms displaying a fibrillar pattern should be considered atypical unless extenuating circumstances account for constant frictional forces (since constant frictional pressure is required to form the fibrillar pattern)
Features of atypical fibrillar pattern (type B) on plantar skin:
- Increased variability in color of fibrillar lines
- Increased variability in thickness of fibrillar lines
- Disorganized distribution (lack of uniform alignment)
- Gray-colored fibrillar lines -- should always be considered atypical
The atypical fibrillar pattern may represent an artifactual expression of the parallel ridge pattern on pressure-loaded areas of the sole, and oblique-view dermoscopy can help differentiate.
4.2.4 Milky-Red Pattern
The milky-red pattern is defined by the presence of homogeneous reddish/whitish colors. This pattern is mainly seen in thicker melanomas that have a nodular component with prominent vascularization. Its presence suggests a more advanced (invasive) lesion.
4.2.5 Multicomponent Pattern
The multicomponent pattern consists of multiple patterns present focally within the lesion, including focal presence of a parallel ridge pattern, furrow pattern, or fibrillar pattern. The focal ridge pattern tends to be found at the periphery of the melanoma.
Additional features of the multicomponent pattern in invasive melanomas:
- Structureless diffuse pigmented areas with multiple colors (brown, red, blue-white, black)
- Irregular dots and globules
- Streaks (serrated edge)
- Irregular blotches
- Blue-white veil
- Regression structures
- Atypical vessels
Advanced invasive ALMs may present with ulceration, symmetry of overall architecture (despite being malignant), and an amelanotic central nodule with clearly visible atypical vessels surrounded by a pigmented periphery showing atypical dots, globules, and parallel ridge pattern.
4.2.6 ALM with Focal Benign Patterns
This is a critically important concept. Melanoma on volar skin may display patterns associated with nevi, including the parallel furrow pattern and lattice-like pattern. However, these benign patterns will be present only focally within the melanoma, with the rest of the lesion displaying malignant patterns (pigmentation on the ridges, diffuse pigmentation with variable shades of colors, atypical fibrillar pattern).
Clinical rule: Malignant patterns trump benign patterns.
When evaluating lesions on volar skin, it is imperative to:
- Search the entire surface area of the lesion for malignant patterns
- Not prematurely anchor the diagnosis based on the focal presence of a benign pattern
- Look for malignant patterns first, then assess for benign patterns
Check Your Understanding
What dermoscopic pattern on acral skin is most specific for melanoma?
The parallel ridge pattern, in which pigmentation follows the ridges (crista superficialis) of the dermatoglyphics, is most specific for acral melanoma. In contrast, benign acral nevi show a parallel furrow pattern where pigment follows the furrows (sulci). The distinction between ridge and furrow pigmentation is the most critical dermoscopic feature on acral skin.
Key Takeaways
- The parallel ridge pattern (pigment on the ridges (crista superficialis) of dermatoglyphics) is the hallmark of acral melanoma and has the highest sensitivity and specificity of any single dermoscopic feature for ALM.
- Parallel ridge pattern corresponds histopathologically to melanocyte proliferation around eccrine duct openings (acrosyringia) on the crista intermedia.
- Any lesion on palms or soles showing parallel ridge pattern should be biopsied regardless of size, clinical appearance, or patient demographics.
Clinical Scenario
A 68-year-old woman presents with an 8 mm pigmented macule on her right sole that she noticed 6 months ago. Dermoscopy reveals linear brown pigmentation on the ridges (parallel ridge pattern) with whitish dots (eccrine duct openings) distributed within the pigmented bands, along with focal areas of irregular blue-gray pigmentation.
What is the diagnosis, and what is the significance of the blue-gray areas?
Acrolentiginous Melanoma (ALM)
The parallel ridge pattern (pigment on the ridges confirmed by eccrine duct openings within the pigmented bands) is the hallmark of acral melanoma with 86% sensitivity and 99% specificity. Any volar lesion showing this pattern requires biopsy. The focal blue-gray areas suggest dermal invasion beyond the in situ stage, as melanoma in situ typically shows only tan-to-brown ridge pigmentation. This lesion likely has an invasive component requiring urgent excisional biopsy and appropriate surgical margins.
4.3 Amelanotic and Advanced ALM
Amelanotic ALM presents a particular diagnostic challenge because it lacks the typical pigmented patterns. Key dermoscopic clues to amelanotic ALM include:
- Atypical vessels -- particularly corkscrew vessels, which are characteristic
- Remnants of pigment -- even small amounts of residual pigment can guide diagnosis
- Hemorrhage and ulceration
- Hyperkeratosis
These vascular and structural clues are often the only features available to suggest the diagnosis in the absence of melanin-based patterns.
4.4 Size Matters: The 7 mm Rule
Most acquired nevi on volar skin are under 7 mm in greatest diameter. Therefore:
- Acquired melanocytic lesions on volar skin that are greater than 7 mm in greatest diameter should raise suspicion for melanoma, independently of the dermoscopic features displayed by the lesion.
- This size criterion serves as an important safety net when dermoscopic patterns are ambiguous or nontypical.
Check Your Understanding
What is the parallel furrow pattern, and what does it indicate?
The parallel furrow pattern consists of pigmented lines following the sulci (furrows) of acral dermatoglyphics. It is the most common dermoscopic pattern of benign acral melanocytic nevi, found in approximately 45% of cases. Variants include the lattice-like pattern, fibrillar pattern, and crista dotted pattern, all of which are considered benign.
Key Takeaways
- The fibrillar pattern shows oblique pigmented lines crossing both furrows and ridges, caused by mechanical shearing forces on the thick stratum corneum of weight-bearing areas.
- Fibrillar pattern can occur in both benign nevi and melanoma; applying counter-pressure or changing the angle of dermoscope application can reveal whether pigment originates from furrows (benign) or ridges (malignant).
- Irregular diffuse pigmentation (structureless brown-black areas) on acral skin without recognizable parallel patterns should be considered suspicious for melanoma.
4.5 Nontypical Pattern and Algorithmic Evaluation
Some volar lesions will not display any of the typical dermoscopy patterns described for nevi or melanomas. When a lesion cannot be classified into recognized benign (patterns 1-6) or malignant (patterns 10-12) patterns, it is classified as having a "nontypical pattern."
For such lesions, Mikoshiba et al. demonstrated that the following features should raise concern for melanoma:
- Asymmetry in the distribution of colors and structures
- Presence of more than two colors
- Blue-white structures
- Vessels
- Dots
- Streaks
- Abrupt edges
Context (age, size, and location) should not be ignored when trying to differentiate nevi from melanomas.
Clinical Scenario
A 55-year-old man presents with a 5 mm pigmented lesion on his left palm. Dermoscopy reveals linear pigmentation confined to the furrows (parallel furrow pattern) with a lattice-like arrangement. There is no ridge pigmentation, no irregular blotch, and the pattern is symmetric in structure and color.
Is this benign or malignant, and how does the BRAAFF algorithm classify it?
Benign Acral Melanocytic Nevus
The parallel furrow pattern (pigment in the furrows, not on the ridges) is the most common benign dermoscopic pattern on volar skin. Using BRAAFF: irregular Blotch = 0, parallel Ridge pattern = 0, Asymmetry of structures = 0, Asymmetry of colors = 0, parallel Furrow pattern = -1, Fibrillar pattern = 0. Total score = -1 (negative). A score of 0 or below favors a benign lesion. However, if this lesion were >7 mm, closer monitoring would be warranted regardless of the benign pattern, as the 7 mm rule increases suspicion for acral melanocytic lesions above this size threshold.
4.6 The BRAAFF Algorithm
flowchart TD
A[Volar Melanocytic<br/>Lesion] --> B{Irregular<br/>Blotch?}
B -->|Yes: +1| C{Parallel Ridge<br/>Pattern?}
B -->|No: 0| C
C -->|Yes: +3| D{Asymmetry of<br/>Structures?}
C -->|No: 0| D
D -->|Yes: +1| E{Asymmetry of<br/>Colors?}
D -->|No: 0| E
E -->|Yes: +1| F{Parallel Furrow<br/>Pattern?}
E -->|No: 0| F
F -->|Yes: -1| G{Fibrillar<br/>Pattern?}
F -->|No: 0| G
G -->|Yes: -1| H[Calculate<br/>BRAAFF Score]
G -->|No: 0| H
H -->|Score >= 1| I[Suspicious for<br/>Acral Melanoma --<br/>Biopsy]
H -->|Score < 1| J[Low Suspicion --<br/>Monitor]
Lallas et al. created the BRAAFF algorithm to assist clinicians in analyzing volar lesions. This algorithm uses both positive and negative criteria, with each criterion weighted by its association strength with nevi or melanoma.
| Code | Criterion | Type | Score |
|---|---|---|---|
| B | Irregular blotch | Positive (anywhere within the lesion) | +1 |
| R | Parallel ridge pattern | Positive (anywhere within the lesion) | +3 |
| A | Asymmetry of structures | Positive (anywhere within the lesion) | +1 |
| A | Asymmetry of colors | Positive (anywhere within the lesion) | +1 |
| F | Parallel furrow pattern | Negative (anywhere within the lesion) | -1 |
| F | Fibrillar pattern | Negative (anywhere within the lesion) | -1 |
Interpretation: A total score of 1 or greater is required for the lesion to be considered suspicious for acral melanoma.
Key features of the BRAAFF algorithm:
- The parallel ridge pattern carries the highest individual weight (+3), reflecting its strong association with melanoma
- Benign patterns (parallel furrow, fibrillar) serve as negative criteria but cannot fully offset positive findings
- Both positive and negative criteria are assessed anywhere within the lesion
- The algorithm incorporates both pattern-based and symmetry-based criteria
Source: Lallas A, et al., Br J Dermatol, 173(4), 1041-1049, 2015.
Check Your Understanding
How should you approach a pigmented acral lesion that shows neither a clear parallel ridge nor parallel furrow pattern?
When the pattern is ambiguous, the multicomponent pattern (multiple unrelated dermoscopic structures) or the irregular diffuse pigmentation pattern should raise suspicion for melanoma. In such cases, consideration of the lesion's clinical features (size >7 mm, asymmetry, recent change) and comparison with the contralateral site are helpful. Biopsy is recommended for any acral lesion with an irregular or unclassifiable dermoscopic pattern.
Key Takeaways
- The multi-component pattern in ALM combines parallel ridge, irregular diffuse pigmentation, and regression areas, indicating advanced melanoma with multiple growth phases.
- Subungual melanoma extends onto acral skin as a periungual pigmentation (Hutchinson sign) and follows acral dermoscopic rules in the periungual area.
- Globulo-streak pattern at the periphery of an acral lesion indicates lateral expansion of melanocytic nests and should raise concern for melanoma even if the center appears benign.
4.7 Nail Apparatus Melanoma (Subungual Melanoma)
While the primary focus of Chapter 8d is volar skin melanoma, ALM also involves the nail apparatus. The following features are relevant to subungual melanoma (covered in greater detail in Module 33: Nails, and Chapter 11b):
Dermoscopic Features of Nail Melanoma
| Feature | Description | Significance |
|---|---|---|
| Longitudinal melanonychia | Pigmented band running length of the nail plate | Starting point for evaluation; may be benign or malignant |
| Irregular band width/spacing | Variable width, color, or spacing of longitudinal lines | Suggests malignancy; benign bands tend to be regular |
| Micro-Hutchinson sign | Periungual pigmentation visible only with dermoscopy | Highly suspicious for subungual melanoma |
| Hutchinson sign | Periungual pigmentation visible clinically (naked eye) | Classic sign of subungual melanoma |
| Destruction of nail apparatus | Partial or complete nail plate destruction | Indicates advanced invasive melanoma |
| Parallel ridge pattern on hyponychium | PRP visible on the exposed hyponychial skin | Corresponds to in situ tumor component in the nail region |
When the nail apparatus is destroyed by invasive melanoma, examination of the hyponychium and surrounding volar skin may reveal the stereotypical parallel ridge pattern, with white eccrine ducts opening on top of the pigmented ridge, corresponding to areas of in situ tumor.
4.8 Differential Diagnosis
4.8.1 Acral Melanocytic Nevus
- Displays benign patterns: parallel furrow, lattice-like, fibrillar, globular, homogeneous, or acral reticular
- Usually under 7 mm in greatest diameter
- Uniform brown coloration
- Symmetric structure and color distribution
- See Module 31 for complete description of benign acral patterns
4.8.2 Subcorneal Hematoma (Black Heel, Talon Noir)
- Pigmentation prominent on the ridges, somewhat mimicking the parallel ridge pattern
- Composed of droplets with smooth margins (not diffuse bands)
- Reddish-black color (not brown)
- Pattern described as "pebbles on the ridges" -- discrete droplets rather than continuous band-like pigmentation
- Often the result of ill-fitting sport shoes or trauma
- Scraping test: Paring down the stratum corneum with a scalpel removes the blood, and the underlying skin appears normal
- Rust-colored parallel ridge pattern after sports activity should prompt consideration of subcorneal hemorrhage
4.8.3 Laugier-Hunziker Syndrome
- Benign acquired mucocutaneous hyperpigmentation
- Can display a parallel ridge pattern mimicking melanoma
- Recognized by the clinical context: multiple small brownish macules on multiple fingers AND lips
- Systematic clinical examination prevents misdiagnosis as melanoma
4.8.4 Peutz-Jeghers Syndrome
- Hereditary mucocutaneous pigmentation syndrome
- Can display parallel ridge pattern on acral skin
- Distinguished by characteristic perioral and buccal pigmentation, intestinal polyposis, and family history
4.8.5 Ethnic Pigmentation
- Benign volar pigmentation in patients with darker skin phototypes
- Can display a parallel ridge pattern
- Context of multiple similar lesions, bilateral symmetry, and clinical history help distinguish from melanoma
4.8.6 Chemotherapy-Induced Pigmentation
- Drug-related volar hyperpigmentation
- Can manifest with a parallel ridge pattern
- History of chemotherapy is the key distinguishing factor
4.8.7 Congenital Nevi
- Can occasionally display a ridge pattern on volar skin
- History of presence since birth or early infancy
- Typically larger and with characteristic clinical features
Key Takeaways
- Acral melanoma must be differentiated from acral nevi (parallel furrow), subcorneal hemorrhage (grows out with nail/skin, satellite globules of blood), and ethnic pigmentation (regular parallel furrow on soles).
- The crista dotted pattern (regular dots on ridges) is a benign variant of acral pigmentation commonly seen in children and should not be confused with parallel ridge pattern.
- Any new pigmented lesion on acral skin in adults over 50 should be evaluated with dermoscopy, as ALM incidence increases with age and early detection dramatically improves prognosis.
5. Acral Pattern Reference Table
Table A: Benign Patterns on Volar Skin
| Pattern | Description | Dermoscopic Appearance | Significance |
|---|---|---|---|
| Parallel furrow pattern | Pigmentation following the furrows (sulcus superficialis) | Linear pigment bands in the furrows; ridges remain unpigmented | Benign -- most common nevus pattern on volar skin |
| Lattice-like pattern | Pigmentation following the furrows plus cross-hatching | Furrow pigmentation with linear bands crossing over the ridge from one furrow to the next (like rungs of a ladder) | Benign -- variant of parallel furrow pattern |
| Fibrillar/filamentous pattern | Fine parallel streaks crossing dermoglyphics tangentially | Parallel fine lines crossing the furrows and ridges at an oblique angle | Benign -- caused by mechanical friction on pressure-bearing areas; benign when uniform in color, thickness, and alignment |
| Globular pattern | Globules not associated with a parallel pattern | Round or oval brown structures without alignment to furrows or ridges | Benign |
| Homogeneous pattern | Light brown amorphous pigmentation | Diffuse, uniform light brown color without discernible structure | Benign -- only in lesions less than 7-10 mm |
| Acral reticular pattern | Pigment network independent of skin markings | Well-defined reticular lines not associated with dermatoglyphics | Benign |
Table B: Malignant Patterns on Volar Skin
| Pattern | Description | Dermoscopic Appearance | Significance |
|---|---|---|---|
| Parallel ridge pattern (PRP) | Linear pigmentation on the ridges (crista superficialis) | Band-like pigmentation on ridges with whitish eccrine duct dots within bands | Malignant -- hallmark of ALM; sensitivity 86%, specificity 99%, PPV 84% |
| Diffuse pigmentation with variable brown | Structureless pigmentation involving ridges and furrows | Diffuse pigmentation with multiple shades of brown obscuring dermatoglyphics | Malignant -- second most common ALM pattern |
| Serrated pattern | Streak-like projections at tumor edge | Jagged, irregular projections (similar to streaks) at the periphery | Malignant -- occasionally seen in ALM |
| Atypical fibrillar pattern (type B) | Disorganized fibrillar lines with color/thickness variability | Fibrillar lines with variable color, variable thickness, disorganized distribution; gray fibrillar lines | Malignant -- any fibrillar pattern on palms is suspicious; gray fibrils always atypical |
| Milky-red pattern | Homogeneous reddish/whitish coloration | Structureless reddish-white areas | Malignant -- indicates thicker, vascularized, invasive melanoma |
| Multicomponent pattern | Multiple patterns and structures focally present | Focal PRP (often peripheral), diffuse multi-colored pigmentation, irregular dots/globules, streaks, blotches, blue-white veil, regression, atypical vessels | Malignant -- indicates invasive melanoma with multiple dermoscopic features |
Table C: Nontypical Pattern Criteria
When a volar lesion cannot be classified into recognized benign or malignant patterns, the following features raise concern for melanoma:
| Feature | Significance |
|---|---|
| Asymmetry of color distribution | Suspicious |
| Asymmetry of structure distribution | Suspicious |
| More than two colors | Suspicious |
| Blue-white structures | Suspicious |
| Vessels | Suspicious |
| Dots | Suspicious |
| Streaks | Suspicious |
| Abrupt edges | Suspicious |
Clinical context (age, size >7 mm, location) should always be integrated into the assessment.
6. Nail Melanoma Features Table
| Feature | Dermoscopic Finding | Benign vs. Malignant |
|---|---|---|
| Regular longitudinal melanonychia | Uniform parallel lines of consistent color, width, and spacing | Benign -- ethnic melanonychia, melanocytic activation |
| Irregular longitudinal melanonychia | Lines with variable width, spacing, color intensity, and disrupted parallelism | Malignant -- subungual melanoma |
| Micro-Hutchinson sign | Periungual pigment visible only by dermoscopy (not clinically) | Highly suspicious for melanoma |
| Hutchinson sign | Periungual pigment visible to the naked eye | Classic melanoma sign |
| Nail plate destruction | Partial or complete loss of nail architecture | Advanced invasive melanoma |
| PRP on hyponychium | Parallel ridge pattern on skin beneath destroyed nail | In situ melanoma component on volar skin of nail region |
| Triangular shape of band | Band wider at the proximal nail fold, narrower distally | Suggests active matrix melanocyte proliferation (suspicious) |
| Multiple colors within band | Brown, black, gray colors within longitudinal band | Suspicious for melanoma |
7. Clinical Pearls
Ridge vs. furrow -- the fundamental question: In every acral pigmented lesion, the first and most important determination is whether pigment is on the ridges or in the furrows. Use eccrine duct openings (regularly spaced whitish dots on the ridges) as your anatomic landmark to orient the dermoglyphics.
Malignant patterns trump benign patterns: ALM can focally display benign patterns (parallel furrow, lattice-like). Always search the ENTIRE lesion for malignant patterns before concluding benignity. Even a small area of parallel ridge pattern in an otherwise benign-appearing lesion should prompt biopsy.
The 7 mm safety net: Any acquired melanocytic lesion on volar skin greater than 7 mm should raise suspicion for melanoma regardless of the dermoscopic pattern. This size criterion provides an additional safety net when patterns are ambiguous.
Gray fibrillar lines are always atypical: While the fibrillar pattern on the sole can be benign when uniform, any gray-colored fibrillar lines should always be considered atypical and suspicious for melanoma.
Fibrillar pattern on palms is concerning: The fibrillar pattern requires constant frictional pressure. While this is common on the sole (weight-bearing), a fibrillar pattern on the palm should be considered atypical unless the patient's occupation or activities provide a clear mechanical explanation.
Subcorneal hemorrhage mimicry: "Black heel" and post-traumatic subcorneal hemorrhage can convincingly mimic the parallel ridge pattern. Look for reddish-black color (not brown), droplet morphology with smooth margins ("pebbles on the ridges"), and perform the scraping test when in doubt. A rust-colored PRP developing after sports is hemorrhage until proven otherwise.
BRAAFF scoring shortcut: Remember that the parallel ridge pattern alone scores +3 in the BRAAFF algorithm, which exceeds the threshold of 1 needed to classify a lesion as suspicious. The PRP alone is sufficient to warrant biopsy.
Amelanotic ALM -- vessels are the key: When ALM lacks pigment, atypical vessels (especially corkscrew pattern), ulceration, and even minimal remnant pigment or hemorrhage become the critical diagnostic clues. A growing, non-healing lesion on the sole with atypical vessels warrants biopsy.
Laugier-Hunziker and Peutz-Jeghers mimicry: Parallel ridge pattern in these syndromes can be mistaken for melanoma. Always examine the patient's lips, oral mucosa, and other fingers. Multiple bilateral acral macules in characteristic distribution points to a syndrome rather than melanoma.
Oblique-view dermoscopy for fibrillar lesions: An irregular fibrillar pattern may be an artifactual expression of the parallel ridge pattern on pressure-loaded areas of the sole. Oblique-view dermoscopy can help resolve the true underlying pattern.
In situ ALM is detectable: Unlike many other melanoma subtypes, ALM in situ frequently displays the parallel ridge pattern with only tan to brown lines and no other features. This means dermoscopy can detect ALM at its earliest, most curable stage -- making systematic examination of acral pigmented lesions highly rewarding.
Nail apparatus destruction: When ALM destroys the nail apparatus, examine the hyponychium and surrounding volar skin. The parallel ridge pattern on hyponychial skin confirms in situ melanoma and can provide the dermoscopic evidence that triggers biopsy of what might otherwise appear to be a nonspecific nail dystrophy.
Clinical Vignettes
Clinical Scenario A 58-year-old woman presents with a 10 mm pigmented macule on the sole of her left foot near the heel. She noticed it approximately 8 months ago and it has been gradually darkening. Dermoscopy reveals broad brown-black bands of pigment aligned along the sulci (ridges) of the dermatoglyphics. Eccrine duct openings (regularly spaced white dots) are visible within the pigmented bands. The pigmented bands are of variable width and color intensity.
What is the most likely diagnosis?
Diagnosis: Acrolentiginous melanoma (in situ) -- parallel ridge pattern.
The parallel ridge pattern (PRP) -- pigment deposited on the ridges (crista superficialis) where eccrine duct openings are located -- is the most specific dermoscopic finding for acral melanoma (99% specificity). The first and most important determination in any acral lesion is whether pigment is on the ridges or in the furrows (Clinical Pearl 1). The lesion exceeds the 7 mm safety threshold for acquired acral melanocytic lesions (Clinical Pearl 3). The BRAAFF algorithm scores +3 for PRP alone, exceeding the biopsy threshold of 1 (Clinical Pearl 7). In situ ALM frequently displays PRP with only tan to brown lines, meaning dermoscopy can detect ALM at its earliest, most curable stage (Clinical Pearl 11). Biopsy is mandatory.
Clinical Scenario A 45-year-old man, an avid basketball player, presents with a 6 mm dark brown-black macule on the ball of his right foot. He noticed it after a game and is concerned about melanoma. Dermoscopy reveals a reddish-black color with droplet-like globules that have smooth margins, arranged along the ridges. The morphology resembles "pebbles on the ridges." No parallel furrow pattern or lattice-like pattern is seen in the underlying skin.
What is the most likely diagnosis?
Diagnosis: Subcorneal hemorrhage ("black heel") mimicking the parallel ridge pattern.
This case illustrates Clinical Pearl 6: subcorneal hemorrhage can convincingly mimic the parallel ridge pattern. The key distinguishing features are the reddish-black color (rather than brown), the droplet morphology with smooth margins ("pebbles on the ridges"), and the clinical context of athletic activity with frictional trauma. A scraping test can confirm hemorrhage by removing the subcorneal blood. A rust-colored PRP developing after sports is hemorrhage until proven otherwise. However, if doubt remains after the scraping test, biopsy should be performed, as subcorneal hemorrhage can coexist with underlying melanoma. Context prevents errors with the parallel ridge pattern (Clinical Pearl from Module 31).
Clinical Scenario A 70-year-old woman presents with a growing, non-healing, pinkish-red nodule on the sole of her right great toe, measuring 8 mm. She denies any pigmentation. Dermoscopy reveals atypical vessels in a corkscrew-like pattern, ulceration, and a milky-red background. No brown or black pigment is visible. Faint remnant hemorrhagic crusting is present at one edge.
What is the most likely diagnosis?
Diagnosis: Amelanotic acrolentiginous melanoma.
This case demonstrates Clinical Pearl 8: when ALM lacks pigment, atypical vessels (especially corkscrew pattern), ulceration, and even minimal remnant pigment or hemorrhage become the critical diagnostic clues. The corkscrew vessels, milky-red background, and ulceration in a growing acral lesion are alarming for amelanotic melanoma. A growing, non-healing lesion on the sole with atypical vessels warrants urgent biopsy. The differential includes pyogenic granuloma, but the acral location, corkscrew vessel pattern, and elderly age favor melanoma. Amelanotic ALM versus benign vascular lesions can be distinguished by the vascular pattern: benign lesions show regular double-line dots flanking ridges, while amelanotic ALM shows random, disorganized vascular patterns (Clinical Pearl 13 from Module 31).
9. Cross-References
| Topic | Reference |
|---|---|
| Chapter 8d: Acrolentiginous Melanoma (full chapter) | Chapter 8d, pp. 196-201 |
| Introduction and volar skin anatomy | p. 196 |
| Pigment distribution: furrows vs. ridges | p. 196 |
| Schematic of benign and malignant acral patterns | pp. 198-199 |
| Parallel ridge pattern examples | pp. 198-199 |
| Laugier-Hunziker syndrome mimicry | p. 199 |
| Subcorneal blood mechanism | p. 199 |
| Black heel / pebbles on ridges | p. 199 |
| Post-traumatic subcorneal hemorrhage with scraping test | p. 200 |
| Diffuse pigmentation pattern (homogeneous pigment) | p. 200 |
| Serrated pattern (peripheral streaks/dots) | p. 200 |
| Advanced invasive ALM with multicomponent pattern | p. 200 |
| Amelanotic ALM with corkscrew vessels | p. 200 |
| BRAAFF algorithm table | p. 201 |
| Key points summary | p. 201 |
| Benign acral dermoscopic patterns (detailed) | Chapter 11b (see Module 31) |
| Fibrillar pattern mechanics and histology | Chapter 11b (see Module 31) |
| Nail apparatus dermoscopy | Chapter 11b (see Module 33) |
| Melanoma overview and other subtypes | Chapter 8a-8c, Chapter 8e |
10. Related Modules
| Module | Title | Relationship |
|---|---|---|
| Module 01 | Introduction and Principles of Dermoscopy | Prerequisite: Equipment, polarized/nonpolarized dermoscopy, and image capture fundamentals |
| Module 03 | Pattern Analysis Revised | Prerequisite: Parallel lines on ridges as Clue #9 to malignancy; "Chaos and Clues" framework; the three no-chaos exceptions including acral ridge pattern |
| Module 07 | TADA and Other Triage Algorithms | Contains overview of the BRAAFF algorithm among other triage systems for comparative understanding |
| Module 21 | Melanoma: Superficial Spreading and Overview | General melanoma dermoscopy context; ALM may share some features (multicomponent pattern, regression, blue-white veil) |
| Module 23 | Lentigo Maligna / Lentiginous Melanoma on Sun-Damaged Skin | Comparison of site-specific melanoma subtypes; LM on sun-damaged facial skin versus ALM on acral skin -- both require site-specific dermoscopic criteria |
| Module 31 | Palms and Soles (Acral Skin) | Key companion module: Detailed anatomy of volar skin, all six benign acral patterns (parallel furrow, lattice-like, fibrillar, globular, homogeneous, acral reticular), histologic basis for pigment distribution, and differential diagnosis of acral lesions (Chapter 11b) |
| Module 33 | Nails (Nail Apparatus Dermoscopy) | Key companion module: Longitudinal melanonychia evaluation, subungual melanoma features, Hutchinson and micro-Hutchinson signs, differential diagnosis of nail pigmentation, and the nail matrix biopsy decision framework |
Module 24 -- Version 1.0 Part of the Dermoscopy Educational Course.
Image Sources & Citations
- DERM12345 (Skin Lesion Dataset with 40 Subclasses): DERM12345: A Large-scale Skin Lesion Image Dataset with 40 Subclasses. Figshare. 2023. License: CC-BY-4.0.