Module 28: Sensitivity and Specificity -- Rules to Avoid Missing Melanoma and Methods to Improve Diagnostic Accuracy
1. Learning Objectives
After completing this module, the learner should be able to:
- Enumerate and apply the seven practical rules designed to minimize the chance of missing a melanoma during dermoscopic examination.
- Explain the concept of the "ugly duckling" sign and the "signature" nevus pattern, and describe how comparative lesion evaluation improves melanoma detection.
- Identify the three strata of diagnostic difficulty for melanoma ("obvious from the doorway," "apparent on close inspection," and "diagnosis by data integration") and describe the appropriate approach for each level.
- Describe the protocols, indications, and criteria for change used in short-term digital dermoscopic monitoring (approximately 3-month follow-up) and long-term total body photography (TBP) surveillance.
- Explain how patient-related factors -- age, skin phototype, UV exposure history, anatomic site, melanoma risk history, and patient concern -- modify diagnostic thresholds and integrate into clinical decision-making.
- Discuss the role of reflectance confocal microscopy (RCM) as an adjunct to dermoscopy for increasing sensitivity and specificity, including its indications, diagnostic accuracy data, and limitations.
- Interpret key diagnostic accuracy metrics (sensitivity, specificity, benign-to-malignant biopsy ratio, number needed to excise) and explain how dermoscopy, sequential digital dermoscopic imaging (SDDI), TBP, and RCM each affect these metrics.
- Recognize the types of melanoma most commonly missed (amelanotic, nodular, nevoid, facial, acral, small-diameter) and the dermoscopic clues that aid their detection.
2. Prerequisites
- Module 27: Differentiation Patterns and Rules -- understanding of the ABCD rule, Menzies method, seven-point checklist, CASH algorithm, pattern analysis, and their comparative diagnostic accuracies (Chapter 9a/9b content).
- Module 01: Introduction and Principles of Dermoscopy -- familiarity with dermoscopic equipment, polarized versus nonpolarized light, and terminology.
- Module 03: Pattern Analysis -- foundational understanding of global patterns, local features, and the systematic approach to lesion evaluation.
3. Key Concepts
3.1 The Dual Benefit of Dermoscopy
Dermoscopy improves both aspects of diagnostic accuracy simultaneously. It increases sensitivity by revealing melanoma-specific features in lesions that appear clinically benign, thereby catching melanomas that would otherwise be missed. It also increases specificity by enabling recognition of benign lesions that clinically mimic malignancy, thereby reducing the number of unnecessary biopsies.
3.2 Sensitivity versus Specificity: Definitions in Context

- Sensitivity measures the proportion of melanomas correctly diagnosed as suspicious and surgically removed. Higher sensitivity means fewer missed melanomas.
- Specificity measures the proportion of benign lesions correctly diagnosed as benign and spared from unnecessary biopsy. Higher specificity means fewer unnecessary excisions.
- In real-world clinical practice, true sensitivity is difficult to calculate because missed melanomas may not be identified and included in the denominator. Similarly, true specificity is extremely high because clinicians remove only a small fraction of the vast number of skin lesions examined.
3.3 Beyond Algorithms: The Integrative Diagnostic Approach
Scoring algorithms (ABCD rule, Menzies method, seven-point checklist, CASH) are valuable but have limitations. None has been updated since original publication despite the identification of newer melanoma-specific structures (shiny white lines, negative network, angulated lines). Some melanomas remain difficult to diagnose even with these tools. An integrative approach that combines clinical inspection, dermoscopy, patient context, monitoring, and ancillary technologies maximizes diagnostic accuracy.
3.4 The Prerequisite Step: Melanocytic versus Nonmelanocytic
All analytically based scoring algorithms require the lesion to first be classified as melanocytic (nevus versus melanoma) or nonmelanocytic (seborrheic keratosis, BCC, SCC, angioma, dermatofibroma). The algorithms for differentiating nevi from melanoma can only be applied once a nonmelanocytic diagnosis has been excluded. This prerequisite step is itself a potential source of error.
4. Core Content
PART I: Chapter 9c -- Rules to Avoid Missing a Melanoma
Seven practical rules have been identified to enhance the ability to detect melanomas, including those that escape detection by conventional algorithmic methods.
4.1 Rule 1: Look at All or As Many Lesions as Possible
Melanoma can clinically mimic a wide range of benign melanocytic and nonmelanocytic skin lesions. Key points include:
- Early melanomas may lack classic clinical ABCD criteria and can resemble benign nevi. Small, flat, macular melanomas may raise no clinical suspicion, yet dermoscopy can reveal clear-cut melanoma features such as asymmetry, irregular globules, and eccentric amelanotic components.
- Thick melanomas (e.g., nodular melanoma) may mimic intradermal nevi, pyogenic granulomas, or dermatofibromas.
- Dermoscopic criteria of melanoma typically become apparent before clinical ABCD criteria manifest, making dermoscopic evaluation of all lesions (not just clinically preselected suspicious ones) essential for maximizing sensitivity.
- In patients with multiple nevi, examining all lesions is the only reliable method for detecting melanomas that morphologically resemble nevi (e.g., nevus-associated melanomas that clinically appear as inconspicuous dermal nevi but reveal asymmetry, serpentine vessels, eccentric hyperpigmentation, and structureless areas on dermoscopy).
- Time burden is minimal: Studies have demonstrated that dermoscopic examination of all nevi adds approximately only 2 minutes to a routine clinical examination.
4.2 Rule 2: Undress High-Risk Patients
Total body skin examination (TBSE) involves a visual inspection of the patient's complete body surface for lesions suggestive of skin cancer. The literature emphasizes:
- American Cancer Society guidelines recommend that skin examination be part of a general periodic health examination.
- Only approximately 30% of dermatologists routinely perform TBSE on all patients.
- Patient factors significantly associated with finding skin cancer on TBSE include: older age, male gender, previous history of nonmelanoma skin cancer, fair skin type, skin tumor as the reason for consultation, and the presence of an equivocal lesion on uncovered areas.
- In younger individuals, the presence of more than 50 melanocytic nevi is one of the strongest risk factors for melanoma. Counting nevi on the arms is a practical screening shortcut: more than 20 nevi on the arms correlates with a high nevus count elsewhere on the body.
TBSE should be offered to at minimum three high-risk groups:
- Patients with a personal history of any skin malignancy or a family history of melanoma in first-degree relatives.
- Patients under 50 years of age with more than 20 nevi on the arms.
- Patients over 50 years of age with evidence of chronic solar damage.
4.3 Rule 3: Use the 10-Second Rule When Evaluating Single Lesions
This rule addresses diagnostic uncertainty as an indicator of suspicion:
- Experienced dermoscopists can usually make a diagnosis in a few seconds because the vast majority of skin neoplasms exhibit repetitive, easily recognized morphologic patterns.
- Even after short training, recognition of stereotypical dermoscopic patterns is usually straightforward.
- A small proportion of lesions, however, lack a pattern typical enough for definitive diagnosis. These cases result in a diagnostic dilemma evidenced by prolonged examination time.
- If a definitive diagnosis cannot be made within 10 seconds of dermoscopic evaluation, the lesion should be considered suspicious due to diagnostic uncertainty.
- Such lesions, if nonpalpable, may be subjected to short-term digital monitoring, but the threshold for biopsy should remain low to maximize early excision of possible melanomas.
Clinical Scenario
A 50-year-old man with a history of dysplastic nevi presents for his annual skin check. Total body examination reveals 60+ nevi, most with a reticular pattern. One 5 mm lesion on his trunk shows a solitary, structureless pink morphology that does not match his signature nevus pattern. Under dermoscopy it is featureless: no network, no globules, no specific structures -- just a pink patch.
What rules guide management of this "featureless" outlier lesion?
Apply the Ugly Duckling Sign and 10-Second Rule
This lesion is a morphologic outlier (ugly duckling sign) that does not match the patient's reticular signature pattern. The 10-second rule states that if you spend more than 10 seconds evaluating a single lesion without reaching a confident benign diagnosis, further action is needed. For a featureless/structureless lesion, options include: (1) short-term digital monitoring (~3 months) to detect subtle change, or (2) biopsy, especially given the patient's melanoma risk profile. The threshold for biopsy should remain low for outlier lesions in high-risk patients.
4.4 Rule 4: Compare and Monitor Multiple Moles
This rule addresses the management of patients with numerous atypical melanocytic nevi:
- Biopsy-all approach: Some clinicians advocate biopsy of all clinically atypical lesions. While safe, this is impractical for patients harboring many atypical nevi.
- Comparative approach with monitoring: A more refined strategy involves excising conspicuous outlier atypical lesions while simultaneously capturing digital images of lesions deemed only slightly atypical, then subjecting those to short-term follow-up (digital monitoring).
Rationale for short-term monitoring:
- Melanomas that cannot be diagnosed clinically or dermoscopically on initial inspection can be diagnosed based on dermoscopic changes observed during follow-up.
- Lesions displaying dermoscopic changes after an average follow-up of approximately 3 months have an 11% probability of being an early, thin melanoma.
- Short-term monitoring thus appears to be an acceptable strategy that maximizes both sensitivity and specificity -- it helps avoid missing melanomas while minimizing excision of benign lesions.
Critical eligibility criteria for monitoring protocols:
Monitoring should ONLY be applied to lesions that are:
- Moderately atypical
- Flat or only slightly raised
- Without a history of change
- Without dermoscopic evidence of melanoma
OR:
- Mildly atypical with a history of change
4.5 Rule 5: Excise Doubtful Nodular Lesions
This rule addresses the particular diagnostic challenge of nodular melanoma:
- Nodular melanoma may lack classic ABCD criteria and may mimic benign tumors including dermal nevi, vascular lesions, dermatofibromas, or seborrheic keratoses.
- Classic dermoscopic criteria of melanoma may be absent because most criteria are based on features observed in superficial spreading melanoma with melanin/melanocytes located primarily in the epidermis or at the dermo-epidermal junction.
Dermoscopic clues for nodular melanoma:
- Blue and black color within the lesion (the "blue-black rule")
- Milky-red areas
- Polymorphous vascular pattern
- Shiny white lines (chrysalis structures)
- Polymorphous vessels and shiny white lines are especially important for amelanotic or hypomelanotic nodular melanomas
Key management principle: Any nodular lesion that does not display diagnostic dermoscopic features associated with a benign diagnosis (e.g., dermatofibroma, intradermal melanocytic nevus, angioma) should be viewed with suspicion, even if it lacks blue-black color, vessels, or shiny white structures.
Nodular lesions should NEVER be subjected to short-term monitoring, because a delay in treatment of even a few months can negatively impact prognosis. For atypical nodular lesions, the guiding principle is: "If in doubt, cut it out!"
4.6 Rule 6: Excise Lesions Revealing Spitzoid Features in Post-Pubertal Patients
- Dermoscopy has dramatically improved the accuracy of diagnosing Spitz nevi, especially the pigmented variant, largely due to the characteristically striking starburst pattern seen in many Spitz nevi.
- However, the starburst pattern may on rare occasions be seen in melanoma.
- In adults, a biopsy should be performed on lesions displaying spitzoid features under dermoscopy. The general rule is to excise spitzoid lesions in post-pubertal patients. This rule serves as a critical safety net, as melanomas may simulate Spitz/Reed nevi both clinically and dermoscopically.
4.7 Rule 7: Combine Clinical, Dermoscopic, and Histologic Criteria
This rule emphasizes the importance of clinico-dermoscopic-histopathologic correlation:
- The index of suspicion for melanoma can sometimes only be raised when dermoscopic features do not confirm the clinical impression.
- A "red flag" should be raised when unexpected features are observed under dermoscopy in the context of clinically banal-appearing lesions.
- Histopathologic examination remains the gold standard for diagnosing melanocytic lesions, but it is not free of limitations or technique failures.
Lesions that may be difficult to interpret histopathologically include:
- Spitzoid tumors
- Lesions exhibiting a high degree of regression
- Nevus-associated melanomas, where the histopathologic diagnosis of melanoma can be missed if a nonrepresentative area of the specimen is evaluated
The importance of providing clinical context to the pathologist:
- Clinically and dermoscopically difficult lesions will often prove to have equivocal histopathology findings, especially if the pathologist is not provided with relevant clinical information.
- Histopathologic reports should always be interpreted in the context of the clinical setting.
- Lesions lacking satisfactory clinico-dermoscopic-histopathologic correlation should be managed with caution.
Check Your Understanding
What is the difference between sensitivity and specificity in the context of dermoscopic algorithms?
Sensitivity is the ability of a dermoscopic algorithm to correctly identify malignant lesions (true positive rate) -- high sensitivity means few melanomas are missed. Specificity is the ability to correctly identify benign lesions (true negative rate) -- high specificity means fewer unnecessary biopsies. There is typically a trade-off between the two.
Key Takeaways
- Sensitivity (proportion of melanomas correctly identified) is the priority in screening settings where missing a melanoma has severe consequences.
- Specificity (proportion of benign lesions correctly identified) determines the biopsy rate; low specificity leads to unnecessary procedures but rarely harms patients.
- Algorithm comparison studies show that dermoscopy improves both sensitivity and specificity over naked-eye examination, with experienced users achieving >90% sensitivity for melanoma.
PART II: Chapter 9d -- Methods to Improve Sensitivity and Specificity in Melanoma Diagnosis
Clinical Scenario
A 42-year-old woman with >100 nevi and a family history of melanoma undergoes total body photography. At her 6-month follow-up, comparative analysis reveals a 4 mm lesion on her right flank that has developed a new eccentric brown area not visible on the baseline image. Dermoscopy shows a reticular pattern with a new focal area of broadened, darkened network lines at one edge.
What monitoring method detected this change, and what is the next step?
Change Detection via Sequential Digital Dermoscopic Imaging (SDDI)
Total body photography with sequential digital dermoscopic monitoring detected a subtle focal change that would have been impossible to identify without baseline comparison. The new eccentric broadened network represents asymmetric morphologic change -- a criterion for excision in digital monitoring protocols. Even small morphologic changes (new structures, focal darkening, asymmetric growth) detected by SDDI warrant biopsy. This approach improves sensitivity for thin melanomas while maintaining specificity by providing objective evidence of change over time.
4.8 The Three Strata of Diagnostic Difficulty
For melanoma, the level of diagnostic difficulty can be stratified into three levels:
Level 1: "Obvious from the doorway"
- Melanoma easily diagnosed by visual inspection alone
- Classic clinical ABCD features: asymmetry, border irregularity, color variegation, diameter greater than 6 mm
- The ugly duckling sign: the outlier lesion that does not follow the pattern of surrounding nevi
- These melanomas will be missed only if overlooked (e.g., hidden from view)
- Patients receiving full skin inspection have a six-fold greater chance of melanoma detection compared with those undergoing only partial examination
- Clinicians should explicitly ask patients about new or concerning lesions, as patients may be reluctant to spontaneously communicate their concerns
Level 2: "Apparent on close inspection"
- Melanoma diagnosable by closely looking at the lesion using clinical and dermoscopic evaluation
- Identified by a chaotic pattern of multiple colors and structures and melanoma-specific criteria
- May be unnoticed with naked eye visualization alone
- May be difficult to spot in a "sea" of multiple pigmented lesions (atypical nevi in high-count patients, or multiple seborrheic keratoses and lentigines in sun-damaged skin)
- Dermoscopic examination of all lesions has been shown to increase sensitivity for detection of suspicious lesions
- Total body photography assists in focusing attention on new or changed lesions among numerous nevi
Level 3: "Diagnosis by data integration"
- The most difficult category: melanomas that cannot be reliably diagnosed on clinical and dermoscopic evaluation alone
- Includes amelanotic, nodular, nevoid, facial, acral, and small-diameter melanomas
- Difficulty arises from lack or scarcity of ABCD criteria (nodular), absence of pigmentation (amelanotic), or scant clinical/dermoscopic criteria (facial)
- Requires integration of multiple data sources (see Section 4.9)
Factors to integrate for "diagnosis by data integration":
- Close-up clinical and dermoscopic examination
- Ugly duckling sign
- Lesion morphology contextualized by patient-related factors
- Melanoma risk per personal and family history
- Patient concern about the lesion
- Total body photography and dermoscopic monitoring
- Reflectance confocal microscopy
- Practical considerations (lesion location, cosmetic sensitivity, lesion count)
None of these factors will always be individually decisive; however, their integration can significantly increase diagnostic accuracy.
4.9 Lesion Morphology by Patient-Related Factors
The morphology of most skin lesions is predictable based on patient-related factors. A lesion that defies the expected morphologic pattern should raise suspicion.
4.9.1 Age
Age significantly impacts the dermoscopic patterns of nevi:
- Childhood: Globular-patterned nevi predominate.
- Adulthood: There is a shift toward predominant reticular pattern.
- Young adults: The peripheral globular pattern correlates with growth. This pattern shows a continuous decrease with every increased decade of age, eventually reaching a frequency of less than 1% after the fourth decade of life.
Clinical implications:
- Globular and peripheral globular patterns are suggestive of benign nevi in younger populations.
- A new globular lesion in later adulthood should not be overlooked.
- In patients greater than 50 years of age, the peripheral globular pattern is quite rare, and strong consideration for biopsy is appropriate.
- New or changing lesions in patients younger than 30 represent far fewer melanomas compared with new or changing lesions in patients older than 50.
- A lower threshold for biopsy should be exercised in the older population group for any new or changing melanocytic lesion.
4.9.2 Skin Type and UV Exposure
- Skin type I: Nevi typically display light brown or pink homogeneous dermoscopic patterns, or reticular pattern with central hypopigmentation.
- Skin type IV: Nevi typically demonstrate dark brown reticular pattern with central hyperpigmentation.
- Pediatric patients with darker skin types: More likely to have reticular nevi of smaller size.
- A lesion that appears darker than the patient's other nevi and is inconsistent with the skin type should be flagged as suspicious.
UV exposure effects on nevi:
- Lesion enlargement
- Darkening or lightening of pigment network
- Erythema
- Appearance of dots, globules, or pigment lamella forming a blotch
- Some changes may be reversible; awareness of phototherapy exposure history should guide evaluation.
4.9.3 Anatomic Site
- Upper back: Higher proportion of globular-patterned nevi.
- Lower back and extremities: Increasing predominance of reticular-patterned nevi centrifugally from the torso.
- The cephalo-caudal transition from globular to reticulated nevi, combined with the higher percentage of globular nevi in the pediatric population, suggests a congenital origin for the globular dermoscopic pattern.
- A new globular-patterned nevus on the lower extremities of an adult should raise suspicion for possible malignancy and warrants biopsy or close monitoring.
4.9.4 "Signature" Pattern of Nevi (Perceived Similarity Clusters)
- Nevi are highly variable between patients but show limited intra-individual diversity.
- Comparative analysis reveals perceived similarity clusters (PSCs) -- the most common pattern of nevi observed in a given patient.
- The mean number of patterns observed per patient is 2.1, which does not differ for patients with atypical nevus syndrome.
- Typically, there is one dominant global dermoscopic pattern (occurring in 40% or more of lesions) and one to two minor patterns (occurring in 20--39% of nevi).
- Recognition of PSCs allows identification of "ugly duckling" nevi that do not bear resemblance to any PSC.
- The sensitivity of the ugly duckling sign for melanoma diagnosis has been demonstrated to be 0.9 (90%) across individuals with different levels of expertise.
- Computerized analysis has corroborated the finding of dermoscopic pattern clustering: 205 randomized nevi from 18 patients were effectively clustered into 18 groups corresponding to the 18 respective patients.
- Evaluation of lesions in context of a patient's other nevi decreases the propensity for unnecessary excision recommendations compared with isolated lesion analysis based purely on morphology.
4.10 Melanoma Risk Per History
The patient's probability of developing melanoma must be weighed into the level of suspicion when evaluating equivocal lesions:
- Patients who have had cutaneous melanoma are at 10-fold increased risk for developing a second melanoma compared with patients without a melanoma history.
- The risk of subsequent melanoma becomes steeper with multiple primaries: one study estimated a 16% probability at year 1 and a 31% chance at year 5 for a third melanoma.
- Second melanomas have been reported to occur at a higher frequency on the same body site as the initial one, particularly when the melanoma occurred on the extremities.
- As many as half of patients with multiple primary melanomas demonstrated similar dermoscopic findings between their melanomas. This was particularly notable among elderly patients with melanomas on sun-damaged skin, featuring pigment network and regression structures.
- This suggests that surveillance should be geared toward the specific dermoscopic features of the patient's prior melanoma(s).
Key Takeaways
- The number needed to biopsy (NNB) for melanoma ranges from 3-5 with expert dermoscopy to 15-30 with naked-eye triage, demonstrating dermoscopy's value in reducing unnecessary excisions.
- Diagnostic accuracy varies by melanoma subtype: highest for SSM, lower for nodular and amelanotic melanoma, requiring subtype-aware evaluation strategies.
- No algorithm achieves 100% sensitivity; the management of equivocal lesions (short-term monitoring vs. biopsy) must consider patient risk factors, clinical context, and lesion trajectory.
4.11 Patient Concern
Patient concern is a valuable input in the diagnostic algorithm:
- More than half of patients (57%) detected their own melanomas, with females showing higher self-detection rates (69%) than males (47%).
- The higher rate of female self-detection is multifactorial: greater knowledge about the disease, greater tendency for skin self-examination, and higher likelihood of having professional skin cancer screening.
- Patients who perform routine self-skin examinations are more likely to be diagnosed with thinner melanomas.
- Increased patient education and encouragement of self-skin examination can be highly beneficial in melanoma detection.
4.12 Total Body Photography (TBP) and Dermoscopic Monitoring
4.12.1 Total Body Photography
- Baseline TBP consists of 12 to 24 high-resolution clinical photographs of a patient's cutaneous surface.
- The premise: melanomas appear as new or changing lesions, while most nevi remain static.
- TBP predominantly increases specificity: an equivocal lesion is reassuringly identified as benign based on long-standing stability compared with previous overview images.
- TBP can also increase sensitivity: an early melanoma may display subtle clinical and dermoscopic features but elicit concern because it is detected as a new or changed lesion (e.g., a nearly amelanotic lesion with scant structureless pigmentation and a few serpentine vessels that proves to have markedly grown over 4 years when compared to TBP).
- TBP has been demonstrated to decrease the benign-to-malignant biopsy ratio -- as low as 3:1 in one study -- since evidence of nevi stability decreases the chance of unnecessary biopsy.
4.12.2 Sequential Digital Dermoscopic Imaging (SDDI)
- SDDI involves the successive capture of dermoscopic images of suspicious skin lesions, allowing evaluation of dermoscopic findings over time.
- SDDI is specifically helpful for detecting melanoma in lesions that lack characteristic clinical and dermoscopic features -- i.e., clinically featureless incipient melanoma.
- By detecting subtle dermoscopic morphologic changes, incipient melanomas without classic dermoscopic changes can be detected earlier.
Diagnostic accuracy data for SDDI:
- One study demonstrated sensitivity of 95.31% and specificity of 99.9%.
- The combination of dermoscopy and SDDI has been shown to double the sensitivity for melanoma and reduce the excision or referral rate of benign lesions by more than 50%.
- Some studies have shown greater efficacy of melanoma detection with TBP compared with SDDI; however, many experts advocate the use of both techniques during surveillance in a "multimodal approach" to increase melanoma diagnostic accuracy.
4.13 Reflectance Confocal Microscopy (RCM)
RCM is a noninvasive diagnostic modality that captures in vivo images at an orientation parallel to the skin surface, offering cellular-level magnification and resolution.
Technical principle: A low-energy diode laser light source is directed toward the lesion. Back-scattering of light, which occurs due to differences in refractive indices within the skin tissue, highlights structures within the lesion. Melanin, keratin, and collagen have a higher refractive index than surrounding tissue, causing these structures to appear particularly white compared with background tissue.
Diagnostic accuracy data:
- A systematic review pooling data from five studies found per-lesion sensitivity of 93% (range 91--97%) and specificity of 76% (range 68--86%) for detection of melanoma.
- The number of lesions needed to excise (NNE) for melanoma detection with RCM as adjunct was 2.4.
Optimal clinical indications for RCM:
- Dermoscopic equivocal lesions where the differential diagnosis is between melanoma and another entity
- Nevi with irregular dermoscopic patterns but clear-cut RCM patterns suggestive of nevi
- Lesions on sun-damaged skin with the differential diagnosis of solar lentigo versus melanoma (RCM can reveal irregular meshwork patterns and "mitochondria-like" elongated junctional nests suspicious for melanoma)
- Lesions with gray-dot granularity under dermoscopy (suggestive of melanophages, as seen in lichen planus-like keratosis, pigmented actinic keratosis, or melanoma)
Settings where RCM is highly reliable:
- Lesions on the head and neck area
- Evaluation of lesions in the setting of chronically sun-damaged skin
- Lesions on the legs
- Lesions with noticeable regression under dermoscopy
Limitation: RCM should not override the clinical and dermoscopic impression given its false negative rate, though this was low at 3.5% in one study.
4.14 Practical Considerations and When to Override Algorithms
- The goal is to increase melanoma detection while maintaining balance through limitation of unnecessary biopsies.
- Number and location of lesions should be considered: removal of one equivocal lesion in a noncosmetically sensitive area can sometimes be the simplest management approach.
- For a lesion suspicious for nodular melanoma, noninterventional observation is not recommended; biopsy should be performed given the potentially aggressive nature of this melanoma subtype.
- Despite the extensive diagnostic tools available, the sensitivity of melanoma detection is not perfect. Patients should therefore be educated on concerning features so they can seek examination sooner if a lesion is not behaving as predicted.
- Algorithms should be overridden when the integration of clinical context, patient risk factors, monitoring data, and ancillary imaging raises sufficient concern, even if the algorithmic score falls below the diagnostic threshold.
4.15 Evidence-Based Recommendations: Integrative Approach
The diagnosis of melanoma is complex, particularly when evaluating melanomas that are not easily identifiable by traditional algorithms. While the delineation of dermoscopic algorithms (seven-point checklist, Menzies method, ABCD rule, CASH) has increased diagnostic accuracy, room for improvement remains.
The recommended integrative approach requires:
- Full-body skin examination combined with dermoscopy of all lesions
- Pooling patient-specific factors (age, skin type, anatomic site, signature nevus pattern)
- Incorporating the patient's melanoma risk per personal and family history
- Considering patient concern and self-detected changes
- Employing diagnostic modalities: TBP, sequential dermoscopic monitoring (SDDI), and RCM as indicated
- Maintaining a low threshold for biopsy when multiple factors converge, even when individual factors are equivocal
Check Your Understanding
What is the 'number needed to excise' (NNE), and how does dermoscopy improve it?
NNE is the number of lesions that must be excised (biopsied) to find one melanoma -- essentially the benign-to-malignant biopsy ratio. Without dermoscopy, NNE is typically 20-40:1. With dermoscopy, NNE improves to approximately 4-10:1, meaning fewer unnecessary biopsies are performed while maintaining or improving melanoma detection.
Key Takeaways
- All validated dermoscopic algorithms perform similarly in meta-analyses, suggesting that the discipline of systematic evaluation matters more than the specific algorithm chosen.
- Training level is the strongest predictor of diagnostic accuracy: structured dermoscopy training improves sensitivity by 15-25% over untrained use of the same instruments.
- Integration of dermoscopy with emerging technologies (AI, reflectance confocal microscopy, total body photography) represents the future direction for maximizing diagnostic accuracy.
5. Monitoring Protocol Reference Table
| Parameter | Short-Term Monitoring (SDDI) | Long-Term Monitoring (TBP) |
|---|---|---|
| Primary purpose | Detect early melanoma in equivocal flat lesions | Identify new or changed lesions over time |
| Typical interval | Approximately 3 months | 6--12 months or longer |
| Image type | Close-up dermoscopic images of individual lesions | 12--24 high-resolution clinical overview photographs of entire body surface |
| Effect on sensitivity | Doubles sensitivity for melanoma when combined with dermoscopy | Primarily increases specificity; can also increase sensitivity by detecting new or changed lesions |
| Effect on specificity | Specificity up to 99.9% reported | Decreases benign-to-malignant biopsy ratio (as low as 3:1) |
| Criteria for change (triggers biopsy) | Asymmetric enlargement, development of new structures (e.g., peripheral streaks), change in pigmentation pattern, any morphologic evolution | Detection of new lesion not present on baseline images; significant change in size, shape, or color of previously documented lesion |
| Eligible lesions | Moderately atypical, flat or only slightly raised, no dermoscopic evidence of melanoma, no history of change (OR mildly atypical with a history of change) | All lesions in high-risk patients |
| Contraindicated for | Nodular lesions (NEVER monitor -- biopsy immediately); lesions with dermoscopic evidence of melanoma; palpable atypical lesions | Not a substitute for dermoscopic evaluation; should not delay biopsy of obviously suspicious lesions |
| Probability of melanoma when change detected | Approximately 11% | Variable; depends on clinical and dermoscopic context |
| Recommended use | Patients with multiple atypical nevi; equivocal flat melanocytic lesions | High-risk patients with multiple nevi, history of melanoma, or atypical nevus syndrome |
6. Diagnostic Accuracy Data Summary Table
| Modality/Technique | Sensitivity | Specificity | NNE / Biopsy Ratio | Key Notes |
|---|---|---|---|---|
| Naked-eye clinical exam | Lower than dermoscopy | Lower than dermoscopy | Higher benign-to-malignant ratio | Full skin inspection yields 6x greater chance of melanoma detection vs. partial exam |
| Dermoscopy alone | Varies by algorithm (62--98%) | Varies by algorithm (35--97%) | Improved over clinical exam | Dual benefit: catches inconspicuous melanomas AND reduces unnecessary biopsies |
| ABCD Rule | 78--98% | 45--80% (experts); 56--78% (nonexperts) | -- | Well-validated; not updated for newer criteria |
| Menzies Method | 86--95% (pigmented); 54% (amelanotic) | 38--76%; 83% (experts) | -- | High sensitivity for pigmented melanoma; lower for amelanotic |
| Seven-Point Checklist | 62--95% (pigmented); 41% (amelanotic) | 35--97% | -- | Wide range; performance varies with expertise |
| Revised Seven-Point Checklist | 88% | 75% | -- | Improved balance |
| CASH Algorithm | 87--98% | 67--68% | -- | Good sensitivity, moderate specificity |
| Pattern Analysis | 82--85% (pigmented); 79--88% (experts) | 61--79%; 68--71% | -- | Preferred by experienced clinicians; superior specificity |
| SDDI (dermoscopy + digital monitoring) | 95.31% | 99.9% | Reduces excision/referral of benign lesions by >50% | Doubles sensitivity when added to dermoscopy |
| TBP | Increases sensitivity for new/changed lesions | Primarily increases specificity | Benign-to-malignant ratio as low as 3:1 | Best for high-risk patients with many nevi |
| TBP + SDDI (multimodal) | Higher than either alone | Higher than either alone | -- | Recommended combined "multimodal approach" |
| Reflectance Confocal Microscopy (RCM) | 93% (range 91--97%) | 76% (range 68--86%) | NNE = 2.4 | Best as adjunct for dermoscopically equivocal lesions |
| Ugly Duckling Sign | 90% (sensitivity = 0.9) | -- | Reduces unnecessary excisions in comparative evaluation | Consistent across different levels of expertise |
7. Clinical Pearls
The 2-minute investment: Adding dermoscopic examination of all nevi to a routine clinical examination adds only approximately 2 minutes but can detect melanomas hiding among clinically inconspicuous lesions. Never preselect only the "suspicious" lesions for dermoscopy.
The 10-second diagnostic threshold: If you cannot arrive at a confident dermoscopic diagnosis within 10 seconds, the lesion itself is telling you something -- treat diagnostic uncertainty as a criterion for suspicion.
Nodular lesions demand action, not observation: Short-term monitoring is never appropriate for nodular lesions. Even a few months' delay can negatively impact prognosis of nodular melanoma. The "if in doubt, cut it out" principle applies specifically and emphatically to raised, nodular, or palpable lesions.
Age-adjusted thresholds: A peripheral globular pattern is normal in young adults but becomes exceedingly rare (less than 1%) after the fourth decade. A new globular lesion in a patient over 50 should prompt strong consideration for biopsy.
The "signature" nevus concept: Each patient has a limited repertoire of nevus patterns (on average 2.1 pattern types). Learning the patient's signature pattern allows the outlier "ugly duckling" to stand out, even if that outlier would appear unremarkable in isolation. The ugly duckling sign achieves 90% sensitivity for melanoma across all expertise levels.
Prior melanomas predict future ones: Patients with a history of melanoma face a 10-fold increased risk of a second primary. Surveillance should be geared toward the specific dermoscopic features of the patient's prior melanoma(s), as half of patients with multiple primaries show similar dermoscopic characteristics between tumors.
Listen to the patient: More than half of melanomas (57%) are self-detected by patients. When a patient expresses concern about a lesion, that concern should be weighted in the diagnostic algorithm, regardless of the lesion's algorithmic score.
The amelanotic trap: Amelanotic and hypomelanotic melanomas are among the most commonly missed. Key clues are polymorphous vascular patterns, milky-red areas, shiny white lines, and the absence of features diagnostic of any specific benign entity.
Spitzoid features in adults are melanoma until proven otherwise: While Spitz nevi classically display the starburst pattern, this pattern can occasionally be seen in melanoma. The general rule is to excise spitzoid lesions in post-pubertal patients.
Correlation is king: Always provide the pathologist with relevant clinical and dermoscopic information. Clinically and dermoscopically difficult lesions tend to have equivocal histopathology, particularly when clinical context is missing. If clinico-dermoscopic-histopathologic correlation is unsatisfactory, manage the lesion with caution.
RCM as tiebreaker, not replacement: RCM is best used for dermoscopically equivocal lesions (sensitivity 93%, specificity 76%, NNE 2.4), but it should not override clinical and dermoscopic impressions given its false negative rate (approximately 3.5%).
Multimodal surveillance for high-risk patients: The combination of TBP and SDDI in a multimodal approach provides the highest diagnostic accuracy for patients with many atypical nevi or a history of melanoma. TBP primarily improves specificity (reducing unnecessary biopsies), while SDDI primarily improves sensitivity (catching incipient melanomas).
Clinical Vignettes
Clinical Scenario A 52-year-old man with a history of melanoma and over 100 nevi presents for routine surveillance. Comparison with TBP from 18 months ago reveals a new 4 mm flat lesion on the left flank. Dermoscopy shows a subtle, featureless light brown structureless pattern. All scoring algorithms classify it as benign.
What is the appropriate management?
Management: Excisional biopsy -- new lesion detected by TBP in a high-risk patient.
TBP identified this lesion as objectively new (Clinical Pearl 12). In a patient over 50 with melanoma history, the appearance of a new melanocytic lesion should lower the biopsy threshold substantially. "Featureless" melanomas are the most commonly missed type.
Clinical Scenario A 45-year-old woman presents with a nearly amelanotic 8 mm pink macule on her upper back. There is scant peripheral light brown pigmentation and a few serpentine vessels. The ABCD score is 3.2 (benign). The 7-point checklist scores 1. She reports it has been slowly growing.
What is the appropriate management?
Management: Excisional biopsy -- the amelanotic trap.
Clinical Pearl 8: amelanotic melanomas are among the most commonly missed. The ABCD score misclassifies this as benign because amelanotic lesions score poorly on color criteria. The revised 7-point checklist scores 1 (biopsy threshold), prioritizing sensitivity. Correlation is king (Clinical Pearl 10): always provide clinical and dermoscopic context to the pathologist.
Clinical Scenario A 38-year-old woman with many atypical nevi has been monitoring a 6 mm flat brown lesion with SDDI. At 3-month follow-up, the lesion shows focal asymmetric darkening with new irregular dots in one quadrant and a 15% increase in diameter. No melanoma-specific structures are visible on standard scoring algorithms.
What is the appropriate management?
Management: Excisional biopsy -- morphologic change detected on SDDI.
Any morphologic change detected through SDDI warrants excision. SDDI primarily improves sensitivity (Clinical Pearl 12) by catching incipient melanomas through documented change before classic features develop. RCM could serve as a tiebreaker (Clinical Pearl 11), but given documented change, biopsy is the most appropriate management.
9. Cross-References
- Chapter 9a: Pattern Analysis and Melanoma-Specific Criteria (pp. 216--219) -- Foundational pattern analysis approach; analytic versus heuristic methods; melanoma-specific structures.
- Chapter 9b: Rules and Algorithms -- ABCD Rule, Menzies Method, Seven-Point Checklist, CASH Algorithm (pp. 220--223) -- Comparative diagnostic accuracy data for scoring algorithms.
- Chapter 4a/4b: Pattern Analysis -- Detailed coverage of global patterns and local features referenced by scoring algorithms.
- Chapter 5c: Figure referenced for monitoring case example (melanoma detected through 1-year follow-up).
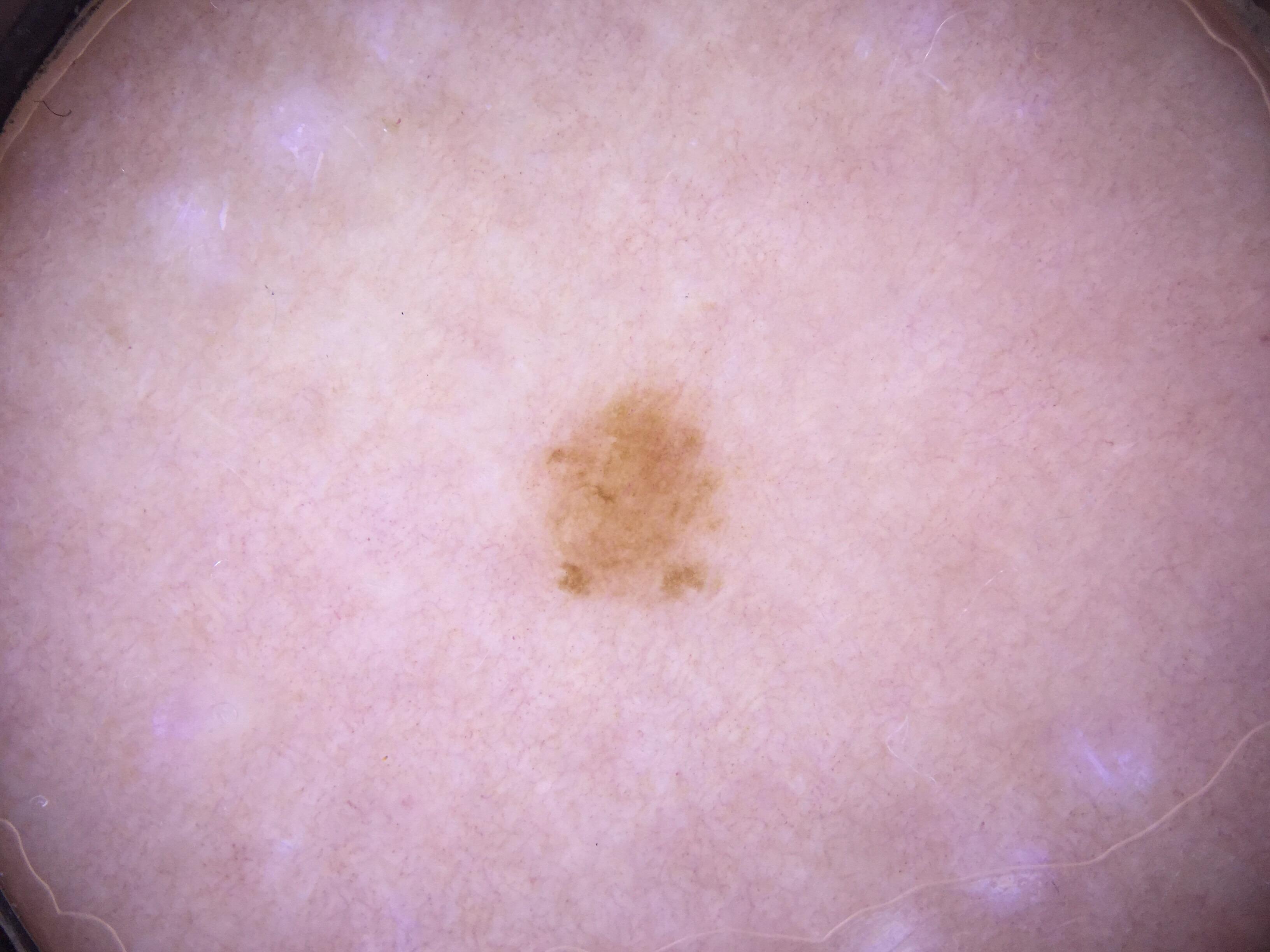
- Early melanoma lacking clinical suspicion but with clear dermoscopic features (asymmetry, irregular globules, eccentric amelanotic component).
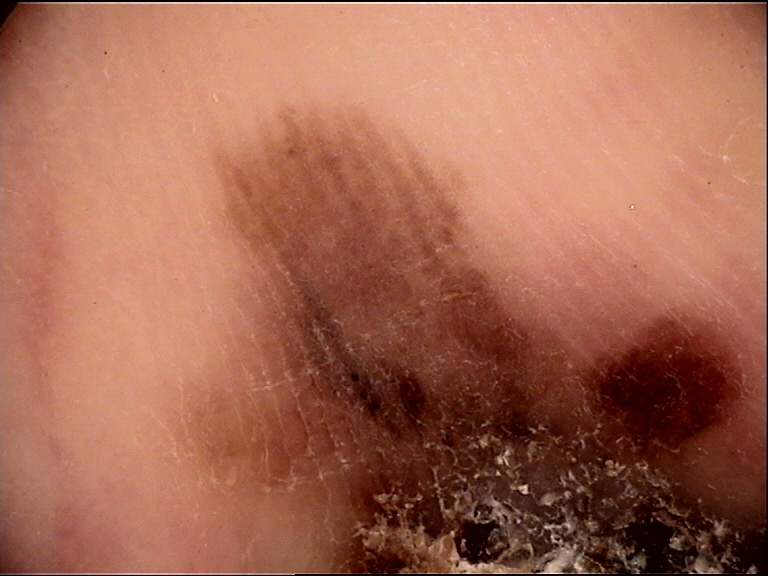
- Featureless lesion on lower back of 75-year-old man (dotted vessels and scaling over pinkish background); no specific features led to excision revealing in situ melanoma.
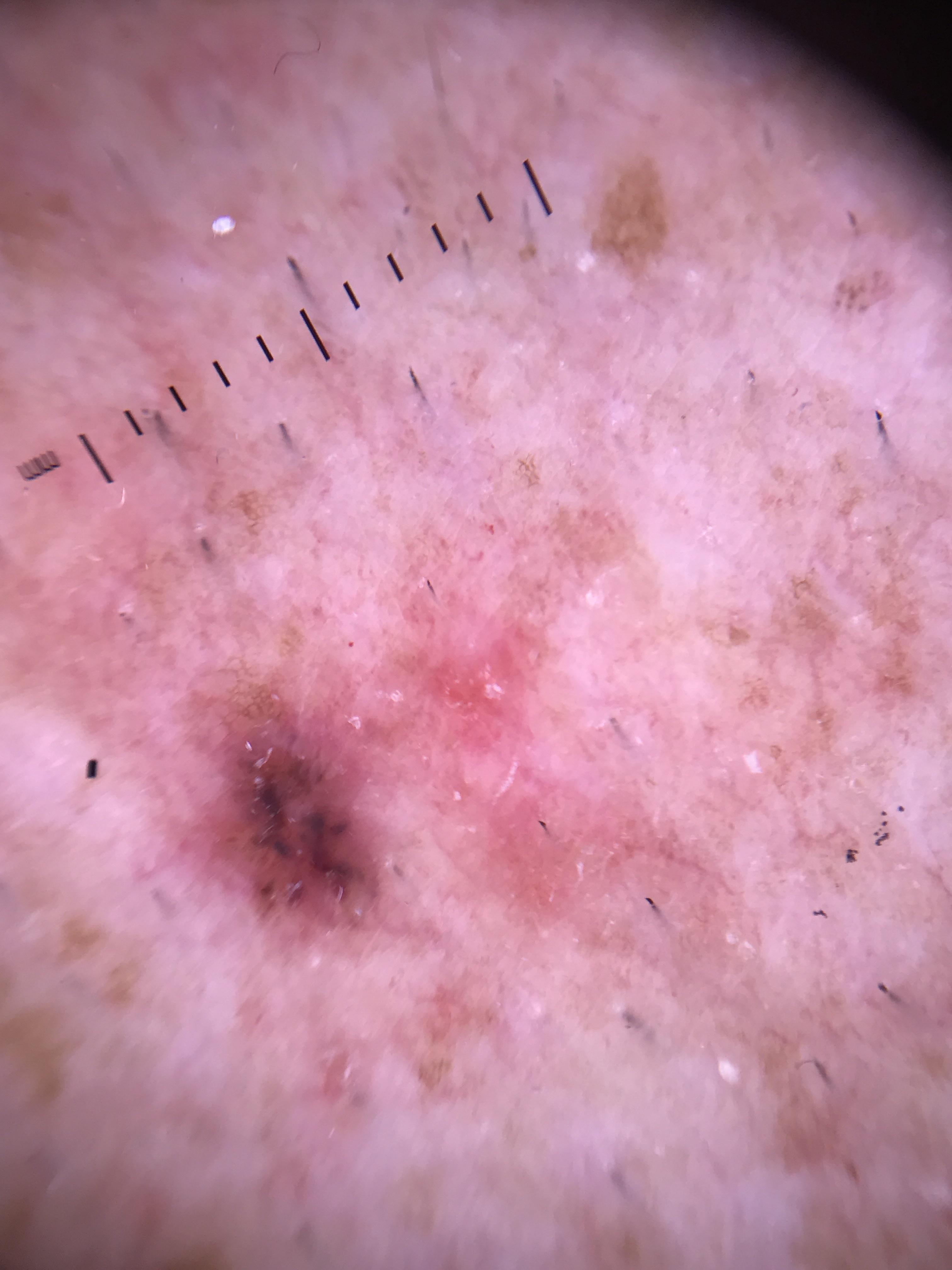
- Nodular amelanotic melanoma examples demonstrating milky-red areas, polymorphous vessels, and whitish areas.
- Melanoma simulating Spitz/Reed nevus with starburst pattern.
- Approach to melanoma diagnosis by diagnostic difficulty (three strata).
- "Doorway" melanoma with classic ABCD features and ugly duckling sign.
- Melanoma in situ diagnosed by data integration -- ugly duckling darker than other lesions and inconsistent with skin phototype.
- Amelanotic melanoma diagnosed by integrating melanoma risk, photographic change, and irregular vessels.
- SDDI case showing pigmentary changes suggestive of melanoma.
- RCM mosaic demonstrating "mitochondria-like" pattern suspicious for melanoma on sun-damaged skin.
10. Related Modules
- Module 27: Differentiation Patterns and Rules -- prerequisite module covering the ABCD rule, Menzies method, seven-point checklist, CASH algorithm, and pattern analysis with comparative accuracy data.
- Module 37: Digital Monitoring -- expanded coverage of SDDI protocols, total body photography workflows, change detection criteria, digital dermoscopy platforms, and long-term surveillance strategies for high-risk patients.
- Module 01: Introduction and Principles of Dermoscopy -- foundational equipment, technique, and terminology.
- Module 03: Pattern Analysis -- detailed global and local pattern recognition essential for applying the rules in this module.
- Module 05: Prediction without Pigment -- relevant to amelanotic/hypomelanotic melanoma detection (vascular patterns, milky-red areas).
Image Sources & Citations
- DERM12345 (Skin Lesion Dataset with 40 Subclasses): DERM12345: A Large-scale Skin Lesion Image Dataset with 40 Subclasses. Figshare. 2023. License: CC-BY-4.0.
- PROVe-AI Dermoscopy Dataset: PROVe-AI: Prospective Validation of AI in Dermatology dataset. License: CC0-1.0.
- HIBA Dermoscopy Dataset: HIBA Dermoscopy Dataset. Hospital Italiano de Buenos Aires. License: CC-BY-4.0.