Module 23: Lentigo Maligna / Lentiginous Melanoma on Sun-Damaged Skin
1. Learning Objectives
After completing this module, the learner should be able to:
- Define chronically sun-damaged skin (CSDS) and describe the histologic epidermal and dermal changes that alter dermoscopic appearances on sun-damaged skin compared with non-sun-damaged skin.
- Describe the clinical presentation of lentigo maligna (LM), including typical location, size, color distribution, border characteristics, and the concept of the "outlier lesion."
- Identify and distinguish the dermoscopic features specific to melanomas on facial CSDS, including annular-granular pattern, asymmetric pigmented follicular openings, angulated lines (zig-zag/rhomboidal structures), circle-within-circle (isobar) pattern, and homogeneous darkly pigmented areas with and without follicular obliteration.
- Apply the facial melanoma progression model (Schiffner model) to classify dermoscopic findings of LM into four sequential stages, from early annular-granular changes through to obliterated follicular openings.
- Recognize the three dermoscopic patterns seen in melanomas on nonfacial CSDS: patchy peripheral pigmented island pattern, granularity/regression pattern, and angulated lines pattern.
- Differentiate LM from its principal simulators -- pigmented actinic keratosis (PAK), solar lentigo, flat seborrheic keratosis (SK), and lichen planus-like keratosis (LPLK) -- using specific dermoscopic criteria.
- Explain the significance of gray color as the single most sensitive dermoscopic feature for LM, while acknowledging its presence in PAK and LPLK as a limitation to specificity.
- Describe the association between LM and desmoplastic melanoma (DM) and explain the importance of lesion palpation in the clinical assessment of suspicious lesions on CSDS.
2. Prerequisites
| Module | Title | Relationship |
|---|---|---|
| Module 01 | Introduction and Principles of Dermoscopy | Required -- understanding of polarized vs nonpolarized dermoscopy, optical principles |
| Module 02 | Histopathologic Correlations of Dermoscopic Structures | Required -- pseudonetwork, regression structures, histopathologic basis of colors |
| Module 03 | Pattern Analysis Revised | Required -- basic dermoscopic elements (lines, dots, clods, circles, structureless areas) |
| Module 30 | Face | Co-requisite -- facial anatomy, pseudonetwork, facial algorithm; may be studied concurrently or immediately after this module |
Assumed Knowledge: Basic skin anatomy (epidermis, dermis, dermal-epidermal junction, adnexal structures), clinical dermatology terminology, melanoma subtypes overview.
3. Key Concepts
3.1 Chronically Sun-Damaged Skin (CSDS)
CSDS refers to skin that has accumulated ultraviolet radiation damage from natural and artificial sources, manifesting clinically as hyperpigmentation, hypopigmentation, mottled pigmentation, telangiectasias, and atrophy (collectively termed poikiloderma). Patients with CSDS present with a spectrum of lesions ranging from benign (lentigines, seborrheic keratoses) through premalignant (actinic keratoses) to malignant (melanoma, nonmelanoma skin cancers).
3.2 Dermoscopy on CSDS -- Why It Looks Different

The histologic changes of CSDS directly alter dermoscopic appearances:
- Epidermal changes: Compacted stratum corneum, flattened rete ridges, cell heterogeneity, vacuolization, reduced Langerhans cells, dysplasia, and zonal necrosis.
- Dermal changes: Solar elastosis with amorphous material, fiber breakdown, scattered macrophages, and coarse granules.
- Dermoscopic consequences: Effacement of the epidermis allows easier visualization of vascular structures and melanophages. Flattened rete ridges eliminate the typical pigment network, producing instead a pseudonetwork formed by pigmented areas interrupted by adnexal/follicular openings.
3.3 Lentigo Maligna (LM) -- Definition
LM is the in situ form of melanoma arising on CSDS (also called Hutchinson melanotic freckle). Both "lentigo maligna" and "lentiginous melanoma on sun-damaged skin" are grouped under the designation LM in this module. Approximately 5% of LM cases progress to invasive melanoma, termed lentigo maligna melanoma (LMM).
3.4 Genetic Background
Melanomas on CSDS are genetically distinct from those on intermittently sun-exposed skin:
| Feature | CSDS Melanoma | Non-CSDS Melanoma |
|---|---|---|
| KIT mutations | 25--28% | 0--2% |
| BRAF mutations | 11--20% | 50--80% |
This has implications for targeted therapy selection.
3.5 The Facial Dermoscopy Challenge
On facial skin with CSDS, the diagnostic challenge is compounded by:
- Absence of a true pigment network (replaced by pseudonetwork)
- High density of pilosebaceous units creating uniform interruptions
- Significant overlap between benign (solar lentigo, SK), premalignant (PAK), and malignant (LM) lesion features
- Many facial lesions co-existing in the same anatomic region
3.6 The "Outlier Lesion" Concept

Despite background CSDS with multiple lentigines and SKs, melanomas on CSDS often appear as isolated, relatively large lentiginous macules that stand out as outlier lesions on visual inspection. Identification of an outlier lesion triggers further dermoscopic examination and is a valuable clinical aid.
4. Core Content
4.1 LM Epidemiology and Natural History
LM is the most common subtype of melanoma on CSDS, followed by superficial spreading melanoma (SSM). Key epidemiologic and natural history features include:
- Location: Most often found on the face, back, and upper extremities.
- Clinical appearance: Brown outlier macules displaying 2--4 colors (most often light brown, dark brown, and pink).
- Borders: Frequently poorly defined.
- Size: Variable; average approximately 9 mm.
- Growth pattern: Slow-growing; LM refers specifically to the in situ form.
- Progression to invasion: Approximately 5% of LM cases progress to LMM (invasive melanoma).
- Histologic subtypes on CSDS: LM is most common, but SSM, nodular melanoma, and desmoplastic melanoma can also arise on CSDS.
4.2 General Dermoscopic Approach to Pigmented Lesions on CSDS
Any pigmented lesion on facial or nonfacial CSDS should first be examined for the presence of melanoma-specific structures applicable to all melanoma subtypes (covered in Chapters 8a--8f):
- Atypical network
- Negative network
- Atypical dots or globules
- Blue-white veil
- Off-centered blotch
- Shiny white structures (polarized light only)
- Peripheral streaks
- Atypical vascular structures (dotted and lineal irregular vessels)
If the lesion does not demonstrate any of these general melanoma-specific structures, a different set of features specific to melanomas on CSDS should be evaluated (described in Sections 4.3 and 4.5).
Check Your Understanding
What is the earliest dermoscopic sign of lentigo maligna on the face?
The earliest sign is asymmetric pigmented follicular openings -- uneven pigment deposition around and within hair follicle ostia. This occurs because atypical melanocytes first proliferate along the follicular epithelium. As the lesion progresses, annular-granular structures (gray dots arranged in rings around follicles) and rhomboidal structures develop.
Key Takeaways
- Lentigo maligna (LM) arises on chronically sun-damaged facial skin and shows an annular-granular pattern of perifollicular gray dots as the earliest dermoscopic sign.
- The pseudonetwork on the face (brown areas interrupted by follicular openings) is the normal background pattern; LM-specific features are superimposed on this pattern.
- Asymmetric pigmented follicular openings (incomplete circles of pigment around follicles) indicate melanocytes extending focally down the hair follicle and are an early LM indicator.
Clinical Scenario
A 75-year-old woman presents with a slowly enlarging 15 mm brown macule on her left cheek that has been present for several years. She has extensive sun damage with multiple solar lentigines. Dermoscopy reveals an annular-granular pattern with perifollicular gray dots, asymmetrically pigmented follicular openings, and focal areas of dark homogeneous pigmentation obliterating some follicular openings.
What is the most likely diagnosis, and what stage does the Schiffner progression model indicate?
Lentigo Maligna (LM)
The annular-granular pattern with perifollicular gray dots is the earliest dermoscopic sign of LM. The asymmetrically pigmented follicular openings indicate melanocytes extending down the hair follicle. The focal follicular obliteration by dark homogeneous pigmentation represents an advanced stage in the Schiffner progression model (Stage 3-4), indicating progression from early annular-granular changes toward invasive potential. Despite the slow growth, biopsy is essential to determine if there is invasive lentigo maligna melanoma (LMM).
4.3 Dermoscopic Features of Melanomas on Facial Skin with CSDS
The following six dermoscopic features are characteristic of melanomas (particularly LM) on facial CSDS. While most commonly seen on the face, they can also appear on nonfacial CSDS.
4.3.1 Annular-Granular Pattern (Follicular/Peri-adnexal Granularity)
- Definition: Slate-gray dots and granules (gray to brown) surrounding adnexal openings.
- Morphology: Tiny gray to brown dots aggregated around hair follicles or adnexal openings.
- Histologic correlate: Gray dots correspond to free melanin in the dermis or within melanophages. Brown dots likely correspond to small aggregates/nests of melanocytes.
- Significance: This is the earliest dermoscopic change in LM, representing the first stage of the facial melanoma progression model.
4.3.2 Asymmetric Pigmented Follicular Openings (APFO)
- Definition: Asymmetric distribution of color (tan-brown to gray) surrounding follicular openings.
- Morphology: Dots (usually gray) aggregated around hair follicles in an asymmetric fashion, forming incomplete circles.
- Histologic correlate: Uneven invasion by melanoma cells located within hair follicles; junctional proliferation of atypical melanocytes with focal extension down one portion of the hair follicle.
- Key distinction: In solar lentigines, perifollicular color is tan-brown and symmetric; in LM, it is often gray and asymmetric.
4.3.3 Angulated Lines (Zig-Zag Pattern / Rhomboidal Structures / Polygonal Lines)
- Definition: Multiple confluent grayish to brown lines forming polygonal shapes around and between follicular openings.
- Morphology: Brown to grayish (rarely black) lines meeting at angles, which may coalesce to form polygonal structures such as rhomboids. The lines can be formed by confluent granules or dots.
- Histologic correlate: Constellation of findings including flattening of the DEJ, pagetoid spread of melanoma, and presence of melanophages in the dermis.
- Clinical importance: May be the only criteria present to indicate malignancy. Early angulated lines associated with asymmetric follicular openings, granularity, or perifollicular dots comprise the earliest stage in the progression model.
4.3.4 Circle-Within-a-Circle (Concentric Isobar Pattern)
- Definition: Concentric pigmented rings encircling each other around follicular openings.
- Morphology: A darker dot located within ostial openings, surrounded by one or more concentric rings of pigmentation.
- Histologic correlate: Increased pigmentation (increased number of melanocytes) in the follicular epithelium together with increased pigmentation in a rete ridge surrounding the follicle. Although rete ridges are not common on the face, they can occasionally be seen around follicles harboring melanoma.
- Significance: When present, this feature is highly suggestive of LM; it is rarely seen in pigmented actinic keratosis.
4.3.5 Homogeneous Darkly Pigmented Areas with Preservation of Adnexal Openings
- Definition: Dark brown, gray, or black pigmentation around adnexal openings, with the follicular openings remaining visible.
- Significance: Represents a more advanced stage of LM progression where pigmentation has increased but follicular structures are still identifiable.
4.3.6 Homogeneous Darkly Pigmented Areas with Follicular/Adnexal Obliteration
- Definition: Dark brown, gray, or black pigmentation or blotch with loss of the adnexal openings.
- Significance: Represents the most advanced stage of LM in the progression model, where the rhomboidal structures become thickened and the hair follicles are obliterated as the melanoma advances.
4.4 The Facial Melanoma Progression Model (Schiffner Model)
The Schiffner progression model describes the sequential dermoscopic evolution of LM on sun-damaged facial skin through four stages. Understanding this model is critical for recognizing both early and advanced LM.
Stage 1: Annular-Granular Structures and Early Angulated Lines
- Dermoscopic features: Slate-gray dots and granules around follicular openings (annular-granular pattern); early short angulated lines; early rhomboid structures.
- What is happening: Melanoma in situ begins as melanocytes proliferate at the DEJ. Gray dots represent free melanin or melanin within macrophages. As dots accumulate around follicles, the annular-granular pattern forms.
- Histologic correlate: Junctional proliferation of atypical melanocytes along the DEJ, with early melanin accumulation in the dermis and within melanophages.
- Clinical note: This is the earliest, most subtle stage. The findings may be focal and require careful examination.
Stage 2: Asymmetric Pigmented Follicular Openings and Rhomboidal Structures
- Dermoscopic features: Asymmetric pigmented follicular openings (grayish hue); rhomboidal structures with perifollicular invasion; short angulated lines coalescing into polygonal shapes.
- What is happening: Melanoma cells within follicles multiply unevenly, creating asymmetric (grayish) pigmentation around follicular openings. Pigmentation begins appearing between follicles (interfollicular changes), forming angulated lines that coalesce into rhomboids.
- Histologic correlate: Junctional proliferation of atypical melanocytes with uneven follicular invasion; early pagetoid spread and melanophages in dermis.
- Clinical note: The transition from perifollicular to interfollicular involvement marks progression. Concentric circle (isobar) patterns may also appear at this stage.
Stage 3: Homogeneous Areas with Preserved Follicular Openings
- Dermoscopic features: Dark homogeneous pigmented areas with preservation of adnexal openings; broadening of rhomboidal structures; possible dark blotches with follicles still visible.
- What is happening: Pigmentation coalesces further. The angulated lines and rhomboids broaden. The follicles are still identifiable but are becoming increasingly surrounded and encroached upon by dense pigmentation.
- Histologic correlate: Advanced junctional proliferation with increasing density of atypical melanocytes along the DEJ and deepening follicular involvement.
- Clinical note: White scarlike areas may be present, representing regression.
Stage 4: Homogeneous Areas with Follicular Obliteration
- Dermoscopic features: Dark brown, gray, or black blotch with obliteration (loss) of adnexal openings; homogeneous structureless dark areas.
- What is happening: The polygonal (rhomboid) structures become thickened and the hair follicles are obliterated as the melanoma becomes more advanced. The adnexal openings are no longer visible within the darkly pigmented blotch.
- Histologic correlate: Dense atypical melanocytic proliferation with extensive follicular and dermal invasion, obliterating normal adnexal architecture.
- Clinical note: This stage represents the most advanced in situ or early invasive phase. Transition to LMM should be considered.
Check Your Understanding
Describe the four progressive stages of dermoscopic evolution in lentigo maligna.
Stage 1: Annular-granular pattern (gray dots around follicles) and early angulated lines. Stage 2: Asymmetric pigmented follicular openings and rhomboidal structures between follicles. Stage 3: Homogeneous darkly pigmented areas with preserved follicular openings. Stage 4: Homogeneous darkly pigmented areas with obliterated follicular openings (complete loss of visible follicles), indicating advanced LM or invasive lentigo maligna melanoma.
Key Takeaways
- Rhomboidal structures (angulated lines forming polygon shapes between follicles) represent pagetoid spread of melanoma cells in the interfollicular epidermis and indicate progression.
- The target-like pattern (dot within a circle around follicles) and concentric circles (isobar pattern) represent increasing melanocyte proliferation around follicular structures.
- Gray circles around follicles indicate junctional proliferation of atypical melanocytes with early follicular and dermal invasion.
4.5 Additional Dermoscopic Features
4.5.1 Gray Pseudonetwork
The pseudonetwork on CSDS facial skin arises because flattened rete ridges eliminate the true pigment network; instead, pigmented areas are interrupted by the high density of adnexal openings. In LM, the pseudonetwork acquires a gray hue due to free melanin and melanophages in the dermis, distinguishing it from the tan-brown pseudonetwork of benign lesions (solar lentigines).
4.5.2 Dark Blotches
As LM advances, pigmentation coalesces into dark blotches. Initially, these blotches still reveal preserved follicular openings (Stage 3), but as melanoma advances, the follicles get obliterated and the blotch becomes a solid dark area (Stage 4).
4.5.3 Target-Like Pattern
The target-like pattern (dot within a circle) is an early perifollicular feature of LM. It consists of a dark central dot surrounded by a circular rim of pigmentation corresponding to melanocytic proliferation at the DEJ around the follicular opening. It is part of the annular-granular spectrum.
4.5.4 Increased Vascular Density
The effacement of the epidermis in CSDS allows easier visualization of vascular structures. Atypical vascular structures (dotted vessels, lineal irregular vessels) may be visible, particularly in more advanced LM or LMM, and should raise concern when seen in conjunction with other LM-specific features.
4.5.5 Gray Color as the Most Sensitive Feature
While the presence of multiple features (granularity, angulated lines, asymmetric follicular openings) increases specificity for LM, the single most sensitive feature is the presence of dermoscopic gray color. Gray color corresponds to free melanin or melanin within melanophages in the upper dermis. However, gray color lacks specificity because it can also be seen in PAK and LPLK.
4.6 Dermoscopic Features of Melanoma on Nonfacial CSDS
Three dermoscopic patterns are seen in up to 78% of melanomas on nonfacial CSDS, in addition to the facial features described above:
4.6.1 Patchy Peripheral Pigmented Island Pattern
- Definition: Peripheral islands of pigment or structureless areas distributed at the periphery in a disorganized manner.
- Description: Toward the center, scarlike areas or hypopigmented areas are seen, with or without the presence of shiny white structures and/or vascular blush. The "islands of pigment" can consist of reticular or structureless areas.
4.6.2 Tan Structureless and Granularity Pattern (Regression Pattern)
- Definition: Areas with regression consisting primarily of gray dots (granularity pattern) combined with tan structureless areas.
- Description: Lesions display a combination of tan structureless areas and gray granularity, suggesting both melanocytic proliferation and regression.
4.6.3 Angulated Lines Pattern
- Definition: Lesions with angulated lines (coalescing into zig-zag lines and polygons), with or without other structures such as granularity or circle-within-a-circle.
- Description: The same angulated lines seen on facial skin can also be present on nonfacial CSDS sites (back, extremities, chest).
- Note: Angulated lines on nonfacial sites may be the only feature indicative of melanoma.
Check Your Understanding
How can dermoscopy help distinguish between actinic keratosis and lentigo maligna on facial skin?
Actinic keratosis shows the strawberry pattern (red pseudonetwork with yellowish follicular plugs) and surface scale, without pigmented follicular involvement. Lentigo maligna shows progressive pigmented changes starting at the follicles (asymmetric follicular openings, annular-granular pattern, rhomboidal structures) without the erythematous background or follicular plugging seen in AK.
Clinical Scenario
A 68-year-old man presents with a 20 mm brown macule on the dorsum of his right forearm (chronically sun-damaged skin). Dermoscopy reveals patchy brown pigmented islands at the periphery, extensive granularity (blue-gray peppering) in the center, and angulated lines forming a zig-zag pattern in one sector.
What is the diagnosis, and what dermoscopic pattern does this represent?
Lentigo Maligna on Nonfacial Chronically Sun-Damaged Skin
This lesion demonstrates all three patterns seen in melanomas on nonfacial CSDS: (1) patchy peripheral pigmented island pattern, (2) granularity/regression pattern in the center, and (3) angulated lines pattern. Gray color (present as blue-gray peppering) is the single most sensitive dermoscopic feature for LM. On nonfacial CSDS, rete ridges are flattened but less effaced than on facial skin, allowing some residual network-like structures (angulated lines). Biopsy is essential for definitive diagnosis.
4.7 LM Melanoma (LMM) -- Invasive Features
Approximately 5% of LM cases progress to invasive LMM. When invasion occurs, the following additional dermoscopic features may appear:
- Blue-white veil: Corresponding to aggregation of heavily pigmented cells in the dermis with compact orthokeratosis.
- Off-centered blotch: Asymmetric dark structureless area.
- Atypical dots or globules: Irregular melanocytic aggregates.
- Shiny white structures: Visible only with polarized dermoscopy; correspond to dermal fibrosis and altered collagen (birefringence).
- Negative network: Serpentine hypopigmented lines surrounding darker islands.
- Atypical vascular structures: Dotted and lineal irregular vessels reflecting neovascularization.
- White scarlike areas: Representing regression/fibrosis.
Clinical pearl -- Palpation: Always palpate any skin lesion on CSDS with suspicious features for melanoma. A firm subcutaneous component may suggest the presence of desmoplastic melanoma (DM), which has a predilection for sun-exposed skin (head and neck) and is associated with an overlying LM in approximately 83% of cases.
Key Takeaways
- Obliterated follicular openings (complete loss of visible follicles within pigmented areas) indicate advanced LM with destruction of adnexal structures by melanoma.
- Progression from LM in situ to invasive LM melanoma is marked by development of blue-gray structureless areas, regression features, and increasingly irregular vessels.
- Blotches with preserved follicles represent dense but noninvasive melanocyte proliferation, while blotches with obliterated follicles indicate tissue-destructive invasion.
4.8 Differential Diagnosis
4.8.1 Pigmented Actinic Keratosis (PAK)
PAK can mimic LM by revealing an annular-granular pattern and structures resembling angulated lines. Key differentiating features:
| Feature | Pigmented AK | Lentigo Maligna |
|---|---|---|
| Follicular openings | Prominent, large, white/pale | Asymmetric, grayish hue |
| Rosettes (polarized) | Multiple rosettes common | Uncommon |
| Line color | Brownish (corresponds to adherent scale) | Grayish to brown |
| Texture on palpation | Rough (adherent scale) | Smooth |
| Borders | Scalloped | Poorly defined |
| Intrafollicular space | Often erythematous ("strawberry pattern") | Gray or brown pigmentation |
| Inner gray halo | Present (associated with PAK) | Uncommon |
| Isobar sign (dot in ostium) | Rarely seen | May be present |
| Scale | Visible on surface | Absent |
4.8.2 Solar Lentigo and Flat Seborrheic Keratosis
Solar lentigines and flat SKs rarely manifest any of the features associated with LM. Key differentiating features:
| Feature | Solar Lentigo / Flat SK | Lentigo Maligna |
|---|---|---|
| Fingerprint-like structures | Present | Absent |
| Moth-eaten borders | Common | Absent |
| Border definition | Well-demarcated | Poorly defined |
| Gyri and sulci | Present (SK) | Absent |
| Perifollicular pigmentation | Symmetric, brown, same hue as surrounding lines | Asymmetric, gray hue |
| Reticular/curved lines | Present | Absent |
| Structureless brown color (uniform) | Common | Replaced by gray-brown |
| LM-specific features | Absent | Present |
Key rule: The presence of solar lentigo/SK features and the lack of any melanoma-specific structures imply a very low likelihood of LM.
4.8.3 Lichen Planus-Like Keratosis (LPLK)
LPLK represents regressing epidermal lesions (SKs and solar lentigines), with abundant dermal melanophages and free melanin appearing as gray dots/granules (peppering). Distinguishing LPLK from LM is one of the most challenging differential diagnoses.
| Feature | LPLK | Lentigo Maligna |
|---|---|---|
| Granule morphology | Coarse-appearing, clumped granules | Fine gray dots |
| Regression direction | Centripetal (from edge inward) | Centrifugal (expanding outward) |
| Edge features | Classic lentigo/SK features visible at lateral edge | No benign features at edge |
| Overall color hue | Often orange hue | Brown hues |
| Other melanoma structures | Absent (only peppering) | May be present |
| Peppering pattern | Expanding centripetally (involution of lentigo/SK) | Expanding centrifugally |
Important caveat: Despite these clues, differentiating LPLK from LM often remains challenging. When confidence is low, biopsy is recommended.
4.8.4 Flat Pigmented Macules -- Exclusion Approach
A lesion on CSDS that does not display diagnostic features of LM and also does not manifest any diagnostic features of AK, lentigo, SK, or LPLK should still be viewed as potential LM. This "diagnosis of exclusion" principle is critical for early detection.
4.9 Margin Mapping with Dermoscopy
Dermoscopy plays a valuable role in the surgical management of LM by guiding biopsy location and margin assessment:
- Biopsy guidance: Areas revealing the most suspicious dermoscopic features (annular-granular structures, asymmetric follicular openings, dots within ostial openings, rhomboidal structures) should be preferentially biopsied to provide the pathologist with the most diagnostically relevant tissue.
- Surgical margin assessment: Dermoscopy can assist in delineating the clinical extent of LM, which is often larger than what is visible to the naked eye, by identifying subclinical features at the periphery of the lesion.
- Caution: When performing a partial (incisional) biopsy, caution should be exercised, as sampling error may miss the most diagnostic areas or areas of invasion.
4.10 Reflectance Confocal Microscopy (RCM) Correlation
Reflectance confocal microscopy is an emerging noninvasive imaging modality that complements dermoscopy in the evaluation of LM:
- RCM can visualize individual cells in vivo at the cellular level, providing near-histologic resolution.
- Studies have demonstrated that RCM improves the histopathologic diagnosis of LM/LMM by guiding biopsy site selection.
- RCM features of LM include pagetoid cells, atypical melanocytes at the DEJ, dendritic cells in the epidermis, and follicular involvement.
- The combination of dermoscopy and RCM increases diagnostic accuracy beyond either modality alone, particularly for equivocal facial lesions.
- RCM is especially useful for margin mapping in LM, helping to define the extent of subclinical disease before surgical excision.
Key Takeaways
- The main differential for LM is pigmented AK/solar lentigo: AK preserves follicular openings with keratotic plugs, while LM shows gray perifollicular structures with progressive follicular destruction.
- Reflectance confocal microscopy can be a valuable adjunct for mapping LM margins when dermoscopy is equivocal, particularly before surgical planning.
- Large facial lentigo maligna melanoma may require staged excision with margin control because of the often indistinct clinical borders on sun-damaged skin.
5. LM Progression Model Reference Table
| Stage | Dermoscopic Feature | Description | Histologic Correlate |
|---|---|---|---|
| Stage 1 | Annular-granular structures; early angulated lines; early rhomboids | Slate-gray dots and granules surrounding follicular openings; short lines meeting at angles | Junctional proliferation of atypical melanocytes at DEJ; free melanin/melanophages in upper dermis |
| Stage 2 | Asymmetric pigmented follicular openings; rhomboidal structures with perifollicular invasion; circle-within-circle (isobar) | Gray-hued asymmetric pigmentation around follicles; angulated lines coalescing into polygons; concentric rings | Uneven follicular invasion by melanocytes; melanocytes in follicular epithelium + rete ridges around follicles; early pagetoid spread |
| Stage 3 | Homogeneous darkly pigmented areas with preserved follicular openings; broadened rhomboids; dark blotches (follicles visible) | Dark brown/gray/black pigmentation surrounding but not replacing adnexal openings | Advanced junctional proliferation; increased density of atypical melanocytes; deepening follicular and dermal invasion |
| Stage 4 | Homogeneous darkly pigmented areas with obliterated follicular openings; structureless dark blotch | Dark brown/gray/black blotch replacing follicular openings entirely | Dense atypical melanocytic proliferation with complete obliteration of adnexal architecture; extensive follicular and dermal invasion |
Key principle: As the melanoma progresses, dermoscopic features evolve from perifollicular changes (around follicles) to interfollicular changes (between follicles) to complete follicular obliteration.
6. LM vs Solar Lentigo Differential Table
| Dermoscopic Feature | Lentigo Maligna | Solar Lentigo |
|---|---|---|
| Color | Gray, dark brown, gray-brown, black | Light to medium brown (uniform) |
| Gray color present | Yes (most sensitive feature) | No |
| Perifollicular pigmentation | Asymmetric, gray hue | Symmetric, tan-brown (same hue as surrounding structures) |
| Fingerprint-like structures | Absent | Present |
| Moth-eaten borders | Absent | Common |
| Border definition | Poorly defined, irregular | Well-demarcated, sharp |
| Reticular/curved lines | Absent | Present (fine lines, fingerprinting) |
| Annular-granular pattern | Present (fine gray dots around follicles) | Absent |
| Angulated lines / rhomboids | Present | Absent |
| Circle-within-circle (isobar) | May be present | Absent |
| Asymmetric follicular openings | Present (gray, asymmetric) | Absent (if present, symmetric and brown) |
| Follicular obliteration | May occur (Stage 4) | Absent |
| Structureless brown areas | Replaced by gray/brown-gray | Common, uniform |
| Gyri and sulci | Absent | May be present (in flat SK overlap) |
| Surface texture | Smooth | Smooth |
| Shiny white structures | May be present (polarized) | Absent |
Clinical rule: The presence of solar lentigo features (fingerprinting, moth-eaten border, well-demarcated border, symmetric brown perifollicular openings) combined with the absence of any LM-specific features implies a very low likelihood of LM.
7. Clinical Pearls
Gray is the alarm color. The presence of dermoscopic gray color is the single most sensitive feature for LM. Any gray hue in a facial or CSDS lesion should prompt heightened suspicion and thorough dermoscopic evaluation.
Angulated lines may be the sole clue. Angulated lines (zig-zag pattern, rhomboidal structures) may be the only dermoscopic criterion present to indicate malignancy. Do not dismiss a lesion that lacks other features if angulated lines are present.
Look for the outlier. On patients with CSDS and multiple lentigines, melanomas often appear as isolated, relatively large macules that are "outlier lesions" -- different in size, color, or shape from the surrounding benign lesions.
Palpate every suspicious lesion. Always palpate CSDS lesions suspected of being LM. A firm subcutaneous nodule may indicate underlying desmoplastic melanoma, which is associated with overlying LM in approximately 83% of cases.
Diagnosis by exclusion. A lesion on CSDS that lacks diagnostic features of LM but also does not demonstrate features of AK, lentigo, SK, or LPLK should still be considered a potential LM. The absence of benign features is itself a red flag.
Asymmetry of follicular pigment is key. In solar lentigines, perifollicular pigmentation is tan-brown and symmetric. In LM, it is gray and asymmetric. This subtle difference is one of the most important early discriminators.
Coarse vs fine granularity. LPLK produces coarse, clumped granules, whereas LM produces fine gray dots. However, this distinction is often subtle, and when uncertain, biopsy is warranted.
Regression direction matters. In LPLK, regression (peppering) proceeds centripetally from the edge inward. In melanoma, peppering/granularity expands centrifugally from the center outward. Centrifugal expansion of gray peppering in a presumed lentigo/SK should raise concern.
Nonfacial CSDS has its own patterns. On the back, chest, and extremities, look for three patterns: patchy peripheral pigmented islands, granularity/regression, and angulated lines. These are present in up to 78% of melanomas on nonfacial CSDS.
The isobar sign favors LM over PAK. A dot within an ostial opening (isobar or circle-within-circle pattern) is rarely seen in PAK but may be present in LM. Its presence in a facial lesion should strongly favor LM.
Rough texture = AK, smooth texture = LM. When clinical appearance is equivocal, palpation for surface texture can help: PAK has a rough surface due to adherent scale, while LM has a smooth surface.
Multiple features increase specificity. While gray color alone is sensitive, combining it with granularity, angulated lines, and asymmetric follicular openings substantially increases diagnostic specificity for LM.
Clinical Vignettes
Clinical Scenario A 73-year-old man presents with a 15 mm slowly expanding brown-gray macule on the left malar cheek. It has been present for approximately 2 years. Dermoscopy reveals slate-gray dots and granules clustered asymmetrically around follicular openings (annular-granular pattern). The follicular openings show asymmetric gray halos. A gray pseudonetwork is present. No angulated lines, circle-within-circle patterns, or obliterated follicles are noted. The surface is smooth to palpation.
What is the most likely diagnosis?
Diagnosis: Lentigo maligna (early-to-intermediate stage in the Schiffner progression model).
Gray is the alarm color for LM (Clinical Pearl 1). The annular-granular pattern -- gray dots and granules clustered asymmetrically around follicular openings -- is the hallmark of LM in its early-to-intermediate stages. The asymmetric gray follicular halos are a key discriminator from solar lentigo, which shows symmetric tan-brown perifollicular pigment (Clinical Pearl 6). The smooth surface texture favors LM over pigmented AK, which would be rough (Clinical Pearl 11). The absence of obliterated follicles suggests the melanoma is still in situ. Multiple features (gray color + granularity + asymmetric follicular openings) together substantially increase specificity for LM (Clinical Pearl 12). Biopsy is mandatory.
Clinical Scenario A 68-year-old woman presents with a 12 mm tan-brown macule on the right temple. Her dermatologist previously diagnosed it as a solar lentigo and monitored it for 3 years. Recently, she noticed subtle darkening in one area. Dermoscopy reveals a predominantly homogeneous brown pseudonetwork with symmetric tan follicular halos across most of the lesion. However, one quadrant shows angulated lines forming a subtle zig-zag pattern and faint gray granularity that is not present elsewhere. No obliterated follicles or circle-within-circle patterns are seen.
What is the most likely diagnosis?
Diagnosis: Early lentigo maligna arising within or adjacent to a solar lentigo.
This case illustrates Clinical Pearl 2: angulated lines may be the sole clue to malignancy. The majority of the lesion retains solar lentigo features (symmetric brown pseudonetwork, tan follicular halos), but the focal area with angulated lines and gray granularity in one quadrant represents early LM. Do not dismiss a lesion that lacks other features if angulated lines are present. This also demonstrates the concept of diagnosis by exclusion (Clinical Pearl 5): the area of concern does not match any benign entity. The key teaching point is that LM often arises on a background of sun-damaged skin with coexisting lentigines, and even focal gray features warrant biopsy.
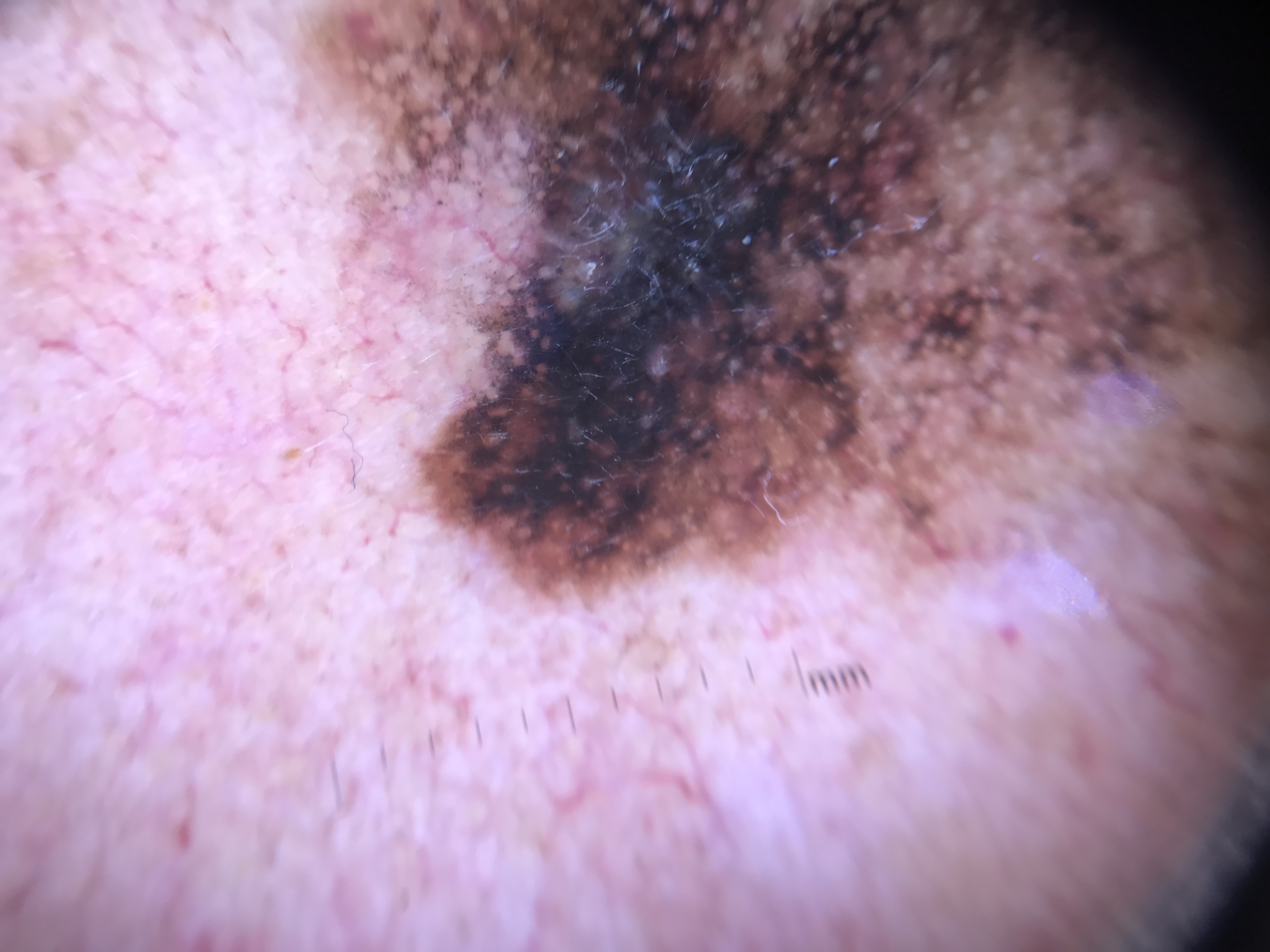
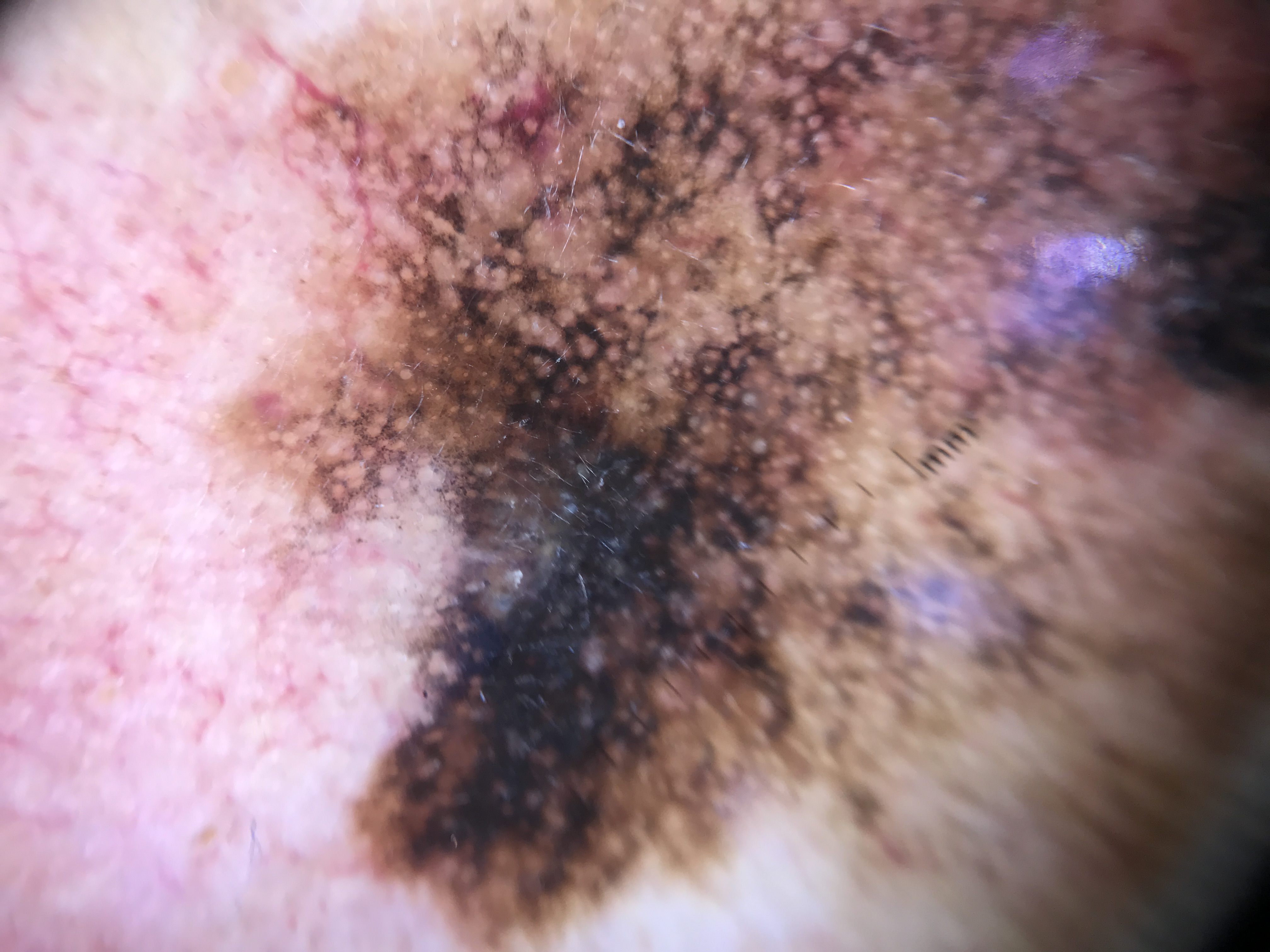
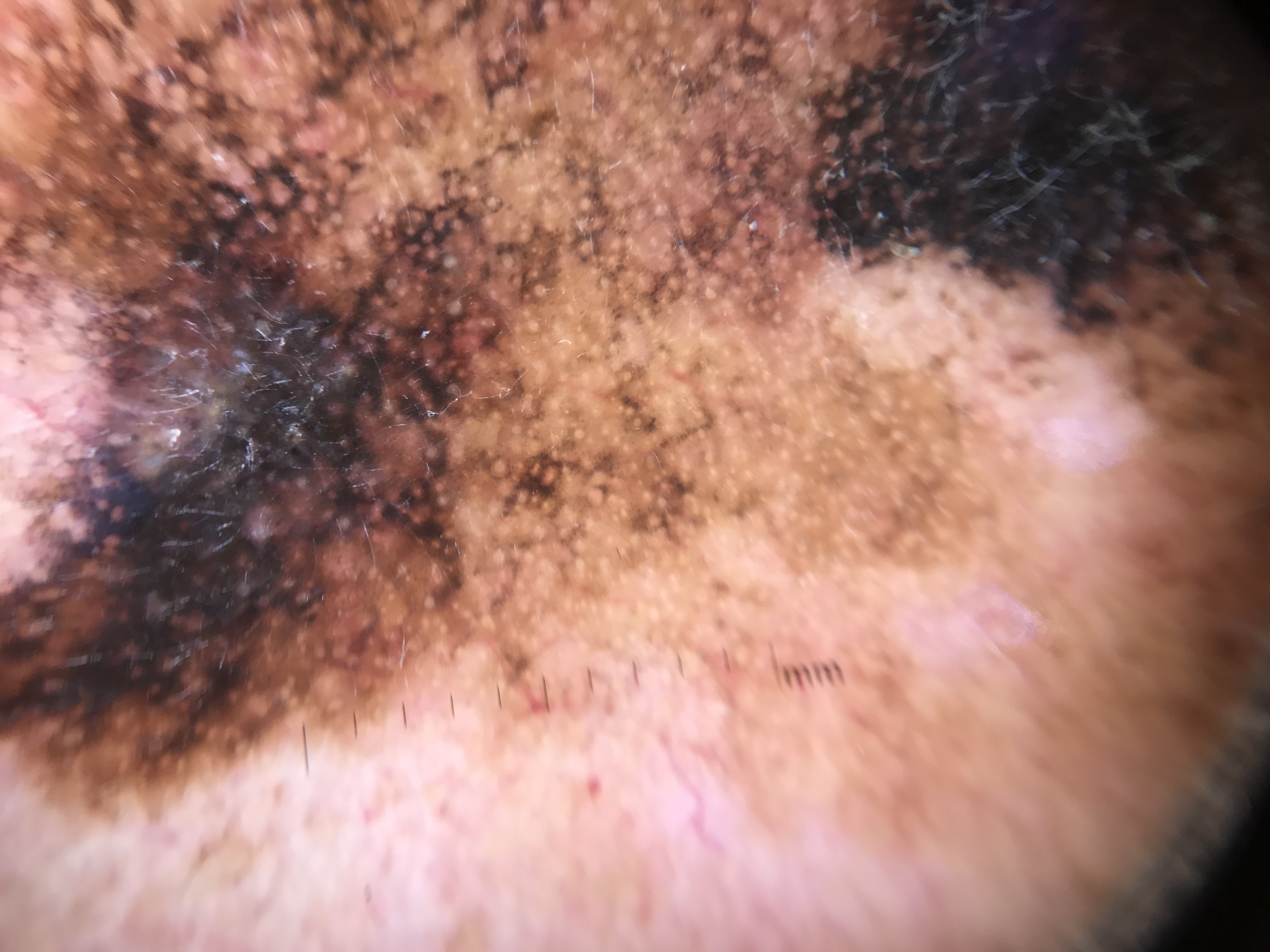
Clinical Scenario An 80-year-old man presents with a large (25 mm) irregularly pigmented patch on the left temple and forehead. Dermoscopy reveals areas of dark brown-black structureless pigment that completely obliterates several follicular openings. A focal area of blue-white veil is present centrally. At the peripheral expanding edge, gray dots are arranged asymmetrically around still-visible follicular openings. Palpation reveals a firm 8 mm area within the patch.
What is the most likely diagnosis?
Diagnosis: Lentigo maligna melanoma (invasive) with possible desmoplastic melanoma component.
This case demonstrates the most advanced stage of the Schiffner progression model. Obliterated follicular openings indicate that the melanoma has progressed beyond the in situ stage (Clinical Pearl 8 from Module 30). The blue-white veil confirms dermal invasion. The peripheral gray perifollicular dots represent the in situ component at the expanding edge. Most critically, the firm palpable area raises concern for an underlying desmoplastic melanoma component -- approximately 83% of desmoplastic melanomas are associated with overlying LM (Clinical Pearl 4). This underscores the importance of always palpating suspicious LM lesions: a firm area mandates deep incisional or excisional biopsy to adequately sample the dermal component.
9. Cross-References
| Topic | Chapter/Section | Relevance |
|---|---|---|
| Histopathologic correlations of facial dermoscopic structures | Chapter 3 | Pseudonetwork, concentric circles, gray circles, asymmetric follicular openings, rhomboids, blotches with obliteration -- histopathologic basis |
| Facial melanoma progression model (Schiffner) | Chapter 11a | Four-stage model with detailed descriptions and figure illustrations |
| Facial melanoma dermoscopic features and algorithm | Chapter 11a | Local features of facial melanoma, differential diagnosis with PAK, LPLK, and pigmented BCC |
| Pigmented actinic keratosis | Chapter 6c/6d | Strawberry pattern, rosettes, inner gray halo, prominent follicles, differential from LM |
| Solar lentigo and seborrheic keratosis | Chapter 6e | Fingerprint-like structures, moth-eaten borders, gyri and sulci, differential from LM |
| LPLK (lichen planus-like keratosis) | Chapter 6e | Granularity, peppering, diffuse vs localized granular patterns, differential from LM |
| Superficial spreading melanoma on CSDS | Chapter 8a | Atypical network, irregular dots/globules -- general melanoma features applicable to CSDS |
| Desmoplastic melanoma | Chapter 8e | Association with overlying LM, firm subcutaneous component, palpation |
| Amelanotic melanoma on face | Chapter 8f | Amelanotic LM features same as amelanotic melanomas elsewhere; atypical vascular patterns |
| Reflectance confocal microscopy | Chapter 9 | RCM for LM diagnosis, biopsy guidance, and margin mapping |
| Management algorithm for facial lesions | Chapter 14 | Stepwise approach to facial pigmented lesion management |
10. Related Modules
| Module | Title | Connection to This Module |
|---|---|---|
| Module 10 | Actinic Keratosis | Pigmented AK is a primary differential for LM; understanding the strawberry pattern, prominent pale follicles, rosettes, and inner gray halo is essential for distinguishing PAK from LM |
| Module 12 | Solar Lentigines, Seborrheic Keratoses, and LPLK | Solar lentigo, flat SK, and LPLK are the other major differentials for LM; fingerprint-like structures, moth-eaten borders, and coarse granularity are key distinguishing features |
| Module 21 | Superficial Spreading Melanoma | SSM is the second most common melanoma on CSDS after LM; general melanoma-specific structures (atypical network, blue-white veil) should be evaluated before LM-specific features |
| Module 22 | Nodular Melanoma | Nodular melanoma can arise on CSDS; atypical vascular patterns and rapid growth are distinguishing features |
| Module 25 | Other Melanoma Subtypes | Desmoplastic melanoma frequently co-occurs with LM (83% of DM cases); palpation is essential |
| Module 26 | Amelanotic and Hypomelanotic Melanoma | Amelanotic LM on the face displays the same vascular features as amelanotic melanomas elsewhere; polymorphous vessels and milky-red areas |
| Module 30 | Face | Co-requisite -- comprehensive coverage of facial dermoscopy anatomy, pseudonetwork, circle-within-circle pattern, facial melanoma vs simulators algorithm, and all facial special-site features |
Image Sources & Citations
- DERM12345 (Skin Lesion Dataset with 40 Subclasses): DERM12345: A Large-scale Skin Lesion Image Dataset with 40 Subclasses. Figshare. 2023. License: CC-BY-4.0.