Module 18: Blue Nevi and Variants
1. Learning Objectives
After completing this module, the learner should be able to:
- Describe the embryologic origin of blue nevi and explain why they appear blue on clinical examination and dermoscopy.
- Recognize the hallmark dermoscopic pattern of common blue nevus -- homogeneous, structureless, steel-blue pigmentation that fades toward the periphery.
- Distinguish the major histopathologic and dermoscopic variants of blue nevi, including common, cellular, combined, compound, sclerotic (desmoplastic), epithelioid, agminated/plaque-type, and deep penetrating nevi.
- Identify additional polarized-light dermoscopic structures (bluish globules/dots, shiny white lines, network-like structures, peripheral out-of-focus streaks) that may be seen in blue nevi.
- Recognize the site-specific features of blue nevi on the face/scalp, palms/soles, and nail apparatus.
- Apply clinical history and dermoscopic criteria to differentiate blue nevi from nodular melanoma, melanoma metastasis, pigmented basal cell carcinoma, vascular lesions, and other blue-lesion mimics.
- Identify the warning signs of malignant blue nevus (blue nevus-like melanoma) and articulate evidence-based indications for biopsy of a blue lesion.
- Describe the role of complementary diagnostic techniques (reflectance confocal microscopy, high-resolution ultrasonography) in the evaluation of blue lesions.
2. Prerequisites
| Module | Title | Why it matters |
|---|---|---|
| Module 01 | Introduction and Principles of Dermoscopy | Foundational understanding of polarized vs. nonpolarized dermoscopy and image acquisition -- essential because polarized light reveals additional structures in blue nevi (shiny white lines, out-of-focus streaks). |
| Module 02 | Histopathologic Correlations of Dermoscopic Structures | Understanding the relationship between colors in dermoscopy and depth of pigment in skin; blue color correlates with deep dermal melanin, the defining feature of blue nevi. |
3. Key Concepts
3.1 Why Lesions Appear Blue

Blue nevi are deep dermal melanocytic proliferations. The blue color seen clinically and dermoscopically is a physical phenomenon: melanin located deep in the dermis (mid-to-deep reticular dermis and occasionally the hypodermis) scatters shorter wavelengths of visible light preferentially toward the observer (Tyndall effect / Rayleigh scattering). The deeper the pigment, the more blue-gray the clinical appearance.
3.2 Embryologic Origin

Blue nevus melanocytes are derived from neural-crest melanocytes that became arrested in the dermis during their migration from the neural crest to the epidermis during embryogenesis. Unlike typical epidermal melanocytes, these cells remain in the dermis and retain dendritic, heavily pigmented morphology.
3.3 Molecular Biology
Somatic mutations in GNAQ and GNA11 (G-protein alpha-subunit genes) have been identified in blue nevi. These same mutations are found in uveal melanoma, providing a molecular link between blue nevi and a specific subset of melanocytic neoplasms.
3.4 Epidemiology
- Prevalence: 1--2% in Caucasians; 3--5% in Asians.
- Age of onset: typically first appear during adolescence and young adulthood, but can also arise in older individuals.
- Preferred locations: distal extensor aspects of limbs (most common), followed by face and scalp, and the sacral region. Less common locations include genitalia, oral cavity, and lymph nodes.
3.5 Defining Histopathology
Common blue nevi show heavily pigmented, bipolar, spindle-shaped melanocytes oriented parallel to the epidermis, intermingled with bundles of collagen in the mid-to-deep dermis, with occasional extensions into the hypodermis. A characteristic grenz zone (a band of uninvolved dermis) is present at the dermo-epidermal junction, devoid of nevomelanocytes.
4. Core Content
4.1 Common Blue Nevus
Clinical Features
- Solitary, small, well-defined, round-to-oval, flat to slightly elevated papule.
- Predominant steel-blue color (spectrum: gray -- blue -- black).
- Most common on distal extensor limbs, face/scalp, and sacral region.
Dermoscopic Features
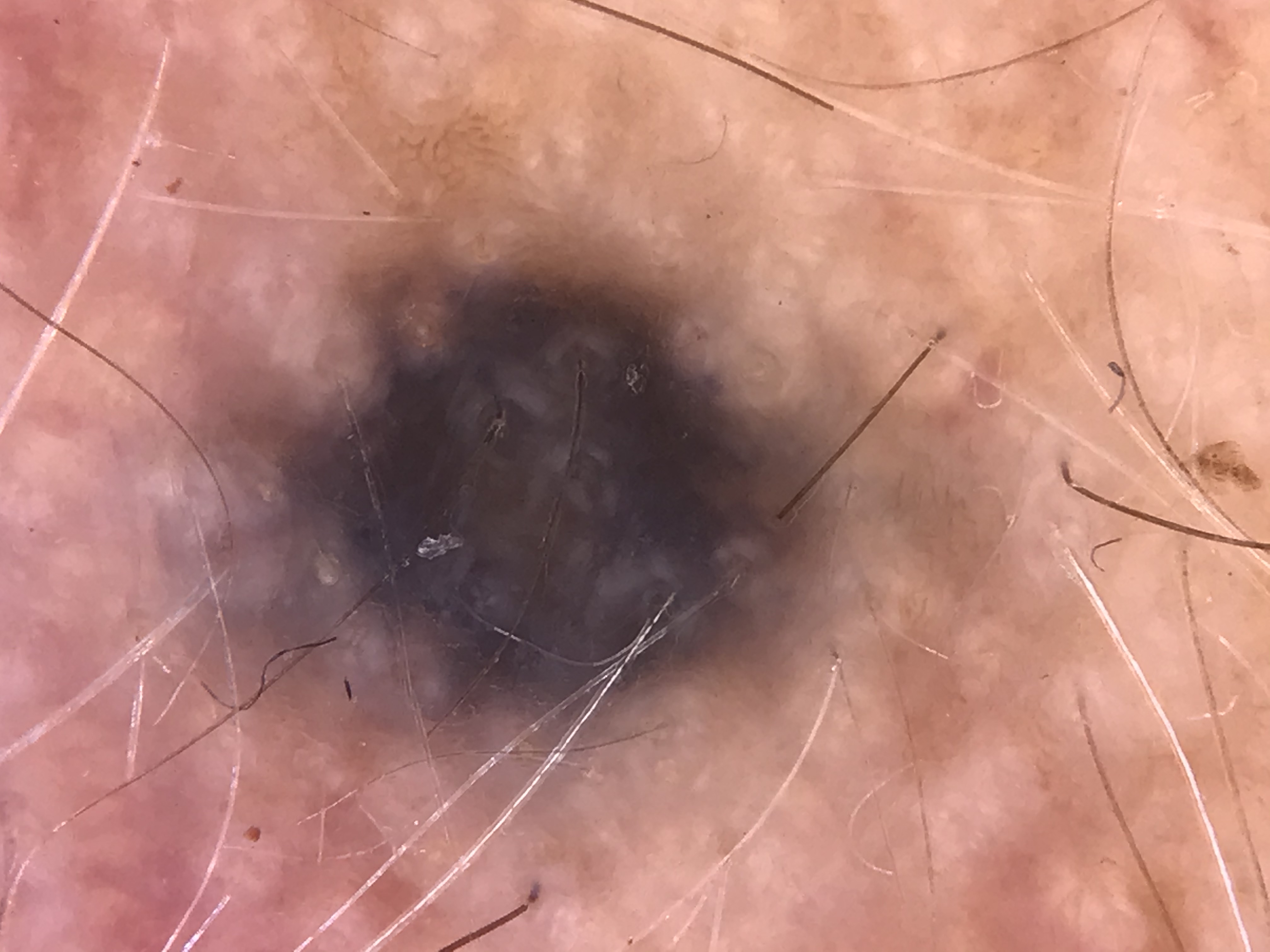
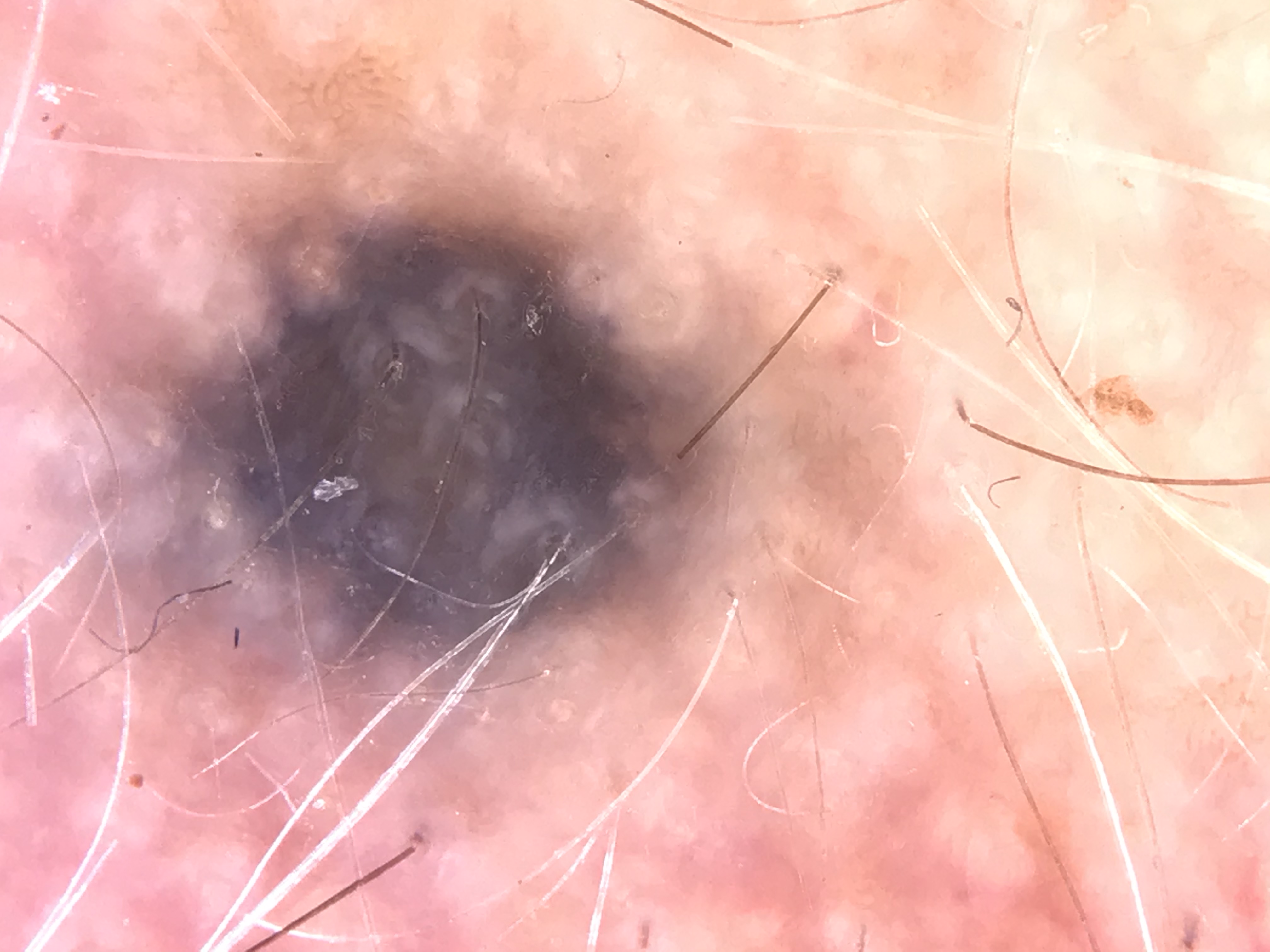
The hallmark dermoscopic pattern is:
- Homogeneous, structureless blue pigmentation -- confluent throughout the lesion.
- Pigment fades gradually toward the periphery (soft, blurred border).
- Color subtypes may include: white-blue, steel-blue-gray, blue-brown, or blue-black. While multichromatic pigmentation can occur, blue is always present in the color spectrum.
Additional Structures Visible with Polarized Dermoscopy
Under polarized light, the following additional structures may be observed:
| Structure | Description | Histopathologic Correlate |
|---|---|---|
| Bluish globules/dots | Small round blue structures | Clusters of pigmented nevomelanocytes in the dermis |
| Shiny white lines | Bright white linear structures visible only with polarized light | Dermal collagen bundles and fibrotic stroma |
| Network-like structures | Faint pigmented network pattern | Pigmented projections of nevomelanocyte clusters |
| Peripheral out-of-focus streaks | Blurred streaks radiating at the periphery | Melanophage or nevomelanocyte clusters extending into surrounding dermis |
Important: Lesions showing more criteria than simple homogeneous structureless blue pigmentation should raise suspicion for melanoma. In such cases, context and clinical history play a critical role in management decisions.
Clinical Scenario
A 27-year-old woman presents with a 4 mm steel-blue, well-defined papule on her left forearm that has been present and unchanged for 8 years. Dermoscopy reveals homogeneous, structureless blue pigmentation that fades gradually toward the periphery with no additional structures.
What is the diagnosis, and what features would raise concern for malignancy?
Common Blue Nevus
The homogeneous structureless blue pigmentation fading at the periphery is the hallmark dermoscopic pattern of a common blue nevus. The long clinical history of stability is reassuring. Features that would raise concern for melanoma include: asymmetric distribution of color, multiple colors beyond blue (white, red, brown in irregular distribution), regression structures, ulceration, blue-white veil with other melanoma-specific structures, or any recent change in size or morphology. A lesion showing more criteria than simple homogeneous blue should prompt biopsy.
4.2 Blue Nevi at Special Sites
Face and Scalp
- Frequently display whitish scar-like areas and follicular white openings.
- Multichromatic pigmentation is more common at this site.
Palms and Soles
- Congenital blue nevi on acral skin displaying a homogeneous blue pattern can be difficult to distinguish from acral melanoma.
- No specific reliable differentiating criteria have been established for this site.
Nail Apparatus
- Rare presentation as blue melanonychia (blue longitudinal pigmented band of the nail).
- No known morphologic dermoscopic criteria reliably distinguish subungual blue nevus from subungual melanoma.
- Any blue melanonychia should be evaluated with a high index of suspicion.
Check Your Understanding
What is the classic dermoscopic pattern of a common blue nevus?
The classic pattern is a homogeneous steel-blue to blue-gray structureless area without any other discernible dermoscopic structures. This pattern results from the deep dermal location of heavily pigmented melanocytes, where the Tyndall effect causes selective scattering of shorter wavelengths, producing the blue color.
Key Takeaways
- Blue nevi show a homogeneous steel-blue structureless pattern corresponding to densely pigmented dendritic melanocytes deep in the dermis.
- The Tyndall effect explains the blue color: melanin deep in the dermis scatters shorter wavelengths preferentially, producing the characteristic blue appearance.
- Common blue nevi are small (typically under 10 mm), well-circumscribed, and stable over time; any change in size, shape, or dermoscopic pattern warrants biopsy.
4.3 Blue Nevus Variants
4.3.1 Cellular Blue Nevus
- Size: Larger than common blue nevus, typically 1--3 cm.
- Location: Usually on the trunk or buttocks.
- Histopathology: Less elongated, slightly pigmented melanocytes with pale cytoplasm forming nevomelanocytic nests in the deep dermis; extension into subcutaneous tissue can be observed.
- Dermoscopy: Structureless blue pigmentation with a white homogeneous center (white areas corresponding to areas of less pigmented cellularity or fibrosis). May appear as a blue-white papule.
4.3.2 Combined Blue Nevus
Combined blue nevus consists of at least two different populations of nevomelanocytes. It is the most common type of "combined nevus" in general.
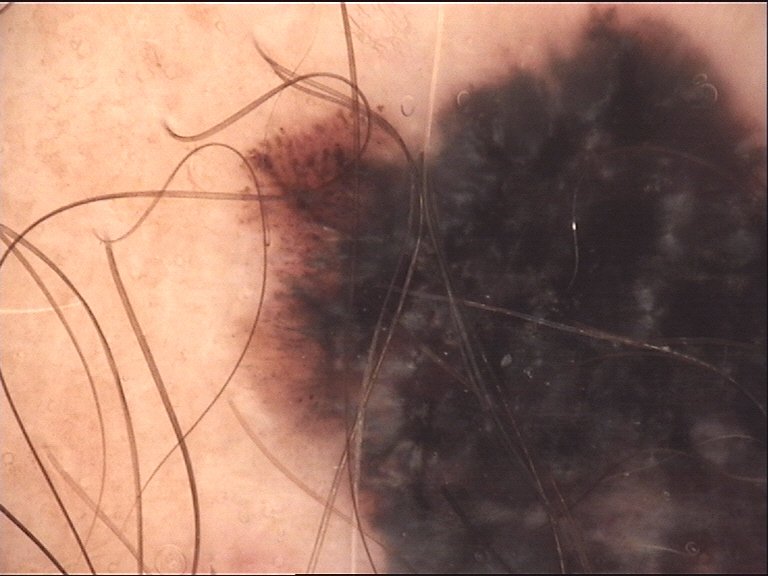
- Most frequent combination: Blue nevus (dermal component) + junctional nevus (at the dermo-epidermal junction).
- Dermoscopy: Central blue-black blotch surrounded by a brown pigment network (the junctional/compound component). This bicomponent pattern is the classic presentation.
- When blue nevus is combined with a dermal or compound nevus: a hypopigmented pattern with brown and blue areas is evident.
- Blue nevi can also be combined with other proliferations, including smooth-muscle hamartomas and trichoepitheliomas.
4.3.3 Sclerotic (Desmoplastic) Blue Nevus
- Dermoscopy: Display whitish areas or whitish scar-like structures corresponding to dermal fibrosis.
- When the scar-like area is located centrally, these lesions can resemble dermatofibromas.
- Histopathology: Bipolar dendritic melanocytes surrounded by prominent sclerotic stroma.
- Amelanotic/hypomelanotic variant: Whitish or gray-whitish structureless pattern with or without thin vessels. This is a rare presentation.
4.3.4 Agminated (Plaque-Type) Blue Nevus
- Presentation: Clustered blue macules or papules arising in an anatomic area measuring less than 10 cm squared.
- Dermoscopy: Multiple structureless confluent blue to gray-black-brown macules or papules.
- The skin surrounding the blue nevi may display a bluish-grayish discoloration or appear completely normal.
4.3.5 Compound Blue Nevus
- Clinical: Small solitary papule.
- Dermoscopy: Symmetric black lamella with a bluish background. Other less common features include dots, globules, or even a pigment network at the periphery.
- Histopathology: Heavily pigmented dendritic melanocytes located both at the dermo-epidermal junction and in the dermis (hence "compound").
- A potential simulator of melanoma.
4.3.6 Epithelioid Blue Nevus
- Describes two distinct clinical settings:
- Pigmented epithelioid melanocytic proliferations occurring in patients with Carney complex (multiple neoplasia and lentiginosis syndrome).
- Blue nevi with a high proportion of polygonal pigmented melanocytes in otherwise healthy individuals.
- No specific dermoscopic patterns have been reported for this variant.
- The Carney complex association warrants systemic evaluation.
4.3.7 Deep Penetrating Nevus
- Considered by some authorities to be a variant of blue nevus.
- Represents a challenging clinical diagnosis due to resemblance to melanoma.
- Dermoscopy: Polychromatic and heterogeneous pattern -- a combination of blue, brown, and whitish pigmentation with possible linear vessels.
- Frequently participates in combined nevi.
4.3.8 Malignant Blue Nevus (Blue Nevus-Like Melanoma)
This term encompasses two distinct entities:
- Melanomas that histologically resemble blue nevi (de novo malignant blue nevus).
- Melanomas arising within pre-existing blue nevi.
Key features:
- Most frequently located on the scalp.
- Tend to grow rapidly and penetrate deeply.
- Molecular profile: May display GNA11 mutations and BAP1 expression loss.
- A new or changing blue lesion in an adult -- especially on the scalp, or in the context of a prior melanoma -- should be viewed with high suspicion.
4.4 Other Diagnostic Techniques
In Vivo Reflectance Confocal Microscopy (RCM)
- RCM improves the diagnostic accuracy of melanocytic tumors generally; however, its maximum depth of visualization is approximately 150 microns.
- Since blue nevus melanocytes are mainly located in the reticular dermis (deeper than 150 microns), RCM is not the ideal instrument for evaluating blue nevi.
- Exception: When the melanocytic proliferation is in the superficial dermis, RCM can reveal nests of hyperrefractile dendritic cells surrounded by collagen fibers.
High-Resolution Skin Ultrasonography (US)
- Has been shown to have higher specificity and similar sensitivity compared to dermoscopy in differentiating blue nevi from cutaneous melanoma metastasis.
- Blue nevi typically appear as dish-shaped, homogeneous, hypoechoic lesions located in the upper dermis.
- Can serve as an adjunct modality when dermoscopy alone is insufficient.
Check Your Understanding
How does a cellular blue nevus differ from a common blue nevus on dermoscopy, and why does it matter?
Cellular blue nevus tends to be larger, may show a multicomponent pattern with white-blue structureless areas, brown globules, or scar-like depigmentation, and can display irregular features. This matters because cellular blue nevus has a small but recognized risk of malignant transformation into blue nevus-like melanoma, and atypical dermoscopic features warrant excision.
Key Takeaways
- Cellular blue nevi are larger, may show heterogeneous blue-brown areas, and carry a low but real risk of malignant transformation (malignant blue nevus).
- Sclerotic (desmoplastic) blue nevi show a lighter blue or white-blue pattern due to dense stromal fibrosis, which can mimic dermatofibroma or BCC.
- Under polarized dermoscopy, blue nevi may reveal shiny white lines corresponding to collagen, which do not change the benign diagnosis but can cause confusion with melanoma.
Clinical Scenario
A 58-year-old man with a history of cutaneous melanoma excised 3 years ago presents with a new 6 mm blue-black nodule on his scalp that appeared 4 months ago and has been growing. Dermoscopy shows a polychromatic pattern with areas of blue, brown, and whitish pigmentation distributed asymmetrically, along with linear vessels.
What is the differential diagnosis, and what is the management priority?
Malignant Blue Nevus (Blue Nevus-Like Melanoma) vs. Melanoma Metastasis vs. Deep Penetrating Nevus
A new, growing blue-black lesion on the scalp of a patient with melanoma history is highly concerning. The polychromatic and heterogeneous pattern with asymmetric color distribution raises suspicion for malignant blue nevus or melanoma metastasis. Deep penetrating nevus can also show polychromatic heterogeneous patterns but is typically stable. Urgent excisional biopsy is mandatory. High-resolution ultrasonography may help differentiate blue nevi (dish-shaped, homogeneous, hypoechoic in upper dermis) from melanoma metastases.
4.5 Differential Diagnosis of Blue Lesions
The evolution or new appearance of a homogeneous blue lesion in a patient with a history of previous invasive melanoma should raise concern for melanoma metastasis.
Key Distinguishing Principles
Melanoma versus Blue Nevus:
- In melanoma, a multichromatic pattern is more frequent.
- Blue pigmentation in melanoma is commonly patchy and is not homogeneously located throughout the lesion.
- The combination of dots/globules + pigment networks, or dots/globules + whitish areas, even with a steel-blue background, is suggestive of melanoma.
Nonmelanocytic Blue Lesion Mimics:
- Other tumors, including basal cell carcinomas, hemangiomas, angiokeratomas, and up to 20% of pilomatrixomas, may present with confluent bluish pigmentation.
- Clinical and dermoscopic clues for each specific entity are typically present to assist in reaching the correct diagnosis.
4.6 When to Biopsy a Blue Lesion
Biopsy should be strongly considered in the following clinical scenarios:
- New blue lesion in an adult -- particularly if appearing after age 40 or growing rapidly.
- Change in a pre-existing blue lesion -- increase in size, change in color, development of asymmetry, or new symptoms (bleeding, itching).
- History of prior invasive melanoma -- any new blue lesion in this context mandates evaluation for possible melanoma metastasis.
- Dermoscopic features beyond simple homogeneous blue -- presence of multiple colors, irregular dots/globules, pigment networks, atypical vessels, milky-red areas, or shiny white streaks suggests malignancy.
- Large size -- blue lesions larger than 1 cm, particularly on the trunk or buttocks (consider cellular blue nevus with potential for atypia).
- Scalp location -- malignant blue nevi have a predilection for the scalp.
- Multichromatic, patchy blue pigmentation -- not homogeneously distributed throughout the lesion.
- Acral or subungual blue lesions -- cannot be reliably distinguished from melanoma by dermoscopy alone.
Key Takeaways
- The primary differential for blue nevus is nodular melanoma; any blue nodule with irregular structure, blue-white veil, peripheral brown globules, or ulceration must be excised.
- Combined nevi (blue nevus component plus another nevus type) may show two distinct dermoscopic patterns and should not be automatically classified as melanoma.
- Tattoo pigment can mimic blue nevus; clinical history of prior tattoo or procedure at the site is essential for correct diagnosis.
5. Blue Nevus Variant Reference Table
| Variant | Typical Size | Preferred Location | Dermoscopic Pattern | Key Histopathologic Feature | Clinical Significance |
|---|---|---|---|---|---|
| Common blue nevus | Small (usually <1 cm) | Distal extensor limbs, face/scalp, sacral region | Homogeneous structureless steel-blue pigmentation fading at the periphery | Heavily pigmented bipolar spindle melanocytes parallel to epidermis in mid-deep dermis; grenz zone at DEJ | Most common type; typically benign and stable |
| Cellular blue nevus | 1--3 cm | Trunk, buttocks | Structureless blue with white homogeneous center | Less elongated, slightly pigmented melanocytes with pale cytoplasm; deep dermal nests extending into subcutis | Larger variant; rarely may undergo malignant transformation |
| Combined blue nevus | Variable | Any site | Central blue-black blotch + peripheral brown pigment network (bicomponent) | Two populations: dermal BN melanocytes + junctional/compound nevus | Most common type of combined nevus overall; mimics melanoma due to asymmetry |
| Sclerotic (desmoplastic) blue nevus | Variable | Face/scalp (commonly) | Whitish scar-like areas + blue pigmentation; blue-white homogeneous pattern | Dendritic melanocytes in prominent sclerotic stroma | May resemble dermatofibroma when scar-like area is central |
| Agminated (plaque-type) blue nevus | Cluster <10 cm squared | Any anatomic area | Multiple confluent blue to gray-black-brown macules/papules | Clustered blue nevi in a defined area | Surrounding skin may show bluish-gray discoloration |
| Compound blue nevus | Small | Any site | Symmetric black lamella with bluish background; +/- peripheral dots, globules, or network | Heavily pigmented dendritic melanocytes at both DEJ and dermis | Potential melanoma simulator |
| Epithelioid blue nevus | Variable | Variable | No specific pattern reported | Polygonal pigmented melanocytes | Association with Carney complex in some cases |
| Deep penetrating nevus | Variable | Face (commonly) | Polychromatic, heterogeneous blue-brown-whitish pigmentation; possible linear vessels | Deep dermal extension with plexiform spindle cell pattern | Challenging diagnosis; often part of combined nevi |
| Malignant blue nevus | Variable, often large | Scalp (predilection) | Additional melanoma features (multicolored, irregular vessels, regression) | Melanoma histology within or resembling blue nevus; GNA11 mutations, BAP1 loss | Rapid growth, deep penetration; requires urgent excision |
6. Blue Lesion Differential Diagnosis Table
| Diagnosis | Key Dermoscopic Features That Distinguish from Blue Nevus | Clinical Clues |
|---|---|---|
| Nodular melanoma | Multiple colors (blue, black, white, brown); atypical vessels; milky-red areas; shiny white streaks. Blue pigmentation is patchy, not homogeneous. | Usually displays rapid growth; may ulcerate; often in adults over 50. |
| Melanoma metastasis | Blue-black pigmentation with white areas; small irregular vessels at the periphery; may be multifocal. | Clinical history of previous invasive melanoma is critical. |
| Pigmented Spitz/Reed nevus | Blue and black colors with starburst pattern, radial streaming, and/or black globules or black network. | Typically younger patients; symmetric starburst pattern. |
| Nodular pigmented BCC | Blue color restricted to ovoid nests, globules, and dots (not diffuse); arborizing vessels; ulceration may be present. | Blue is in discrete nests, not homogeneously distributed. |
| Kaposi sarcoma | Blue-reddish coloration; the "rainbow pattern" (multicolored iridescence). | Clinical presentation; may be multifocal; association with immunosuppression or HHV-8. |
| Hemosiderotic dermatofibroma | Structureless bluish pigmentation (mimics BN closely); fine peripheral pigmented network; shiny white streaks centrally; peripheral vessels. | Often on lower extremities; positive dimple sign on lateral compression. |
| Pilomatrixoma | Irregular white areas; shiny white streaks; reddish homogeneous area; hairpin and irregular vessels. | Up to 20% can display confluent bluish pigmentation; firm subcutaneous nodule. |
| Radiotherapy tattoo | Clinical history of radiation therapy; typical morphology (small, round, blue-black dot); multiple lesions in the radiation field. | Location within known irradiated field; stable over time. |
| Angiokeratoma | Black lacunae with lighter blue color; white interlacing areas separating the lacunae. | Vascular origin; may bleed with trauma; often multiple. |
| Congenital melanocytic nevus | May display homogeneous blue areas combined with other nevus patterns (globules, network); larger size; may have hypertrichosis. | Present since birth; often larger than acquired blue nevi. |
7. Clinical Pearls
"Blue means deep": In dermoscopy, blue color reflects melanin located in the mid-to-deep dermis. A homogeneous, structureless blue pattern that fades at its borders is the sine qua non of common blue nevus. When other structures are present alongside blue pigmentation, the diagnosis of benign blue nevus should not be assumed without further investigation.
History is paramount for blue lesions: A blue lesion present since childhood with no change is reassuring for blue nevus. A new blue lesion in an adult, or any blue lesion in a patient with a history of melanoma, demands heightened suspicion and, usually, biopsy.
The "more than blue" rule: When dermoscopy reveals features beyond simple homogeneous blue pigmentation -- dots/globules combined with pigment network, atypical vessels, milky-red areas, or multiple colors in a patchy distribution -- think melanoma, not blue nevus.
Scalp location is a red flag: Malignant blue nevi (blue nevus-like melanomas) have a predilection for the scalp. Any blue lesion on the scalp that is new, growing, or has heterogeneous dermoscopic features warrants biopsy.
Blue nevi and dermatofibromas can look alike: Sclerotic blue nevi with central whitish scar-like areas closely mimic dermatofibromas. Check for the lateral compression dimple sign (positive in dermatofibromas) and look for the characteristic fine peripheral network of dermatofibromas.
Melanoma metastasis mimicry: In a patient with a history of invasive melanoma, any new blue-black lesion -- especially near a previous excision site -- should be evaluated as a potential melanoma metastasis until proven otherwise. Small irregular vessels at the periphery are an additional warning sign.
Nail blue nevus is a diagnostic blind spot: Blue melanonychia due to subungual blue nevus cannot be reliably differentiated from subungual melanoma dermoscopically. The threshold for referral and biopsy should be low.
GNAQ/GNA11 mutations connect blue nevi to uveal melanoma: The shared molecular pathway underscores the biologic distinctiveness of the blue nevus lineage and informs emerging therapeutic approaches for rare malignant transformations.
Ultrasonography as an adjunct: When dermoscopy is equivocal for differentiating blue nevus from melanoma metastasis, high-resolution skin ultrasonography can add value -- blue nevi typically appear as dish-shaped, homogeneous, hypoechoic lesions confined to the upper dermis.
Combined blue nevi are the most common combined nevi: The combination of a dermal blue nevus component with a junctional or compound nevus produces the classic bicomponent pattern (central blue-black + peripheral brown network). Recognizing this as a combined nevus, rather than melanoma with a blue-whitish veil, is a key dermoscopic skill.
Clinical Vignettes
Clinical Scenario A 30-year-old woman presents with a 5 mm blue papule on the dorsum of the right hand that she says has been present since her teenage years with no change. Dermoscopy reveals a homogeneous, structureless steel-blue pigmentation that fades gradually toward the periphery without an abrupt border. No dots, globules, pigment network, vessels, or additional structures are identified.
What is the most likely diagnosis?
Diagnosis: Common blue nevus.
This is the prototypical presentation of a common blue nevus: a homogeneous, structureless blue pattern that fades at its borders (Clinical Pearl 1). The "blue means deep" principle applies -- the blue color reflects melanin located in the mid-to-deep dermis. The long history since adolescence with no change is reassuring (Clinical Pearl 2). The absence of any additional dermoscopic structures beyond simple homogeneous blue pigmentation is the key finding that confirms this as a benign blue nevus. If features beyond simple blue pigmentation were present -- dots/globules, pigment network, atypical vessels, or multiple colors in a patchy distribution -- the diagnosis of benign blue nevus should not be assumed (Clinical Pearl 3: the "more than blue" rule).
Clinical Scenario A 35-year-old man presents with an 8 mm lesion on the upper back. Dermoscopy reveals a central homogeneous blue-black structureless area occupying approximately 40% of the lesion, surrounded by a peripheral zone of brown pigment network with regular mesh and line characteristics. The transition between the two zones is relatively well-demarcated. No regression structures, irregular streaks, or atypical vessels are visible.
What is the most likely diagnosis?
Diagnosis: Combined blue nevus (blue nevus + junctional/compound nevus).
Combined blue nevi are the most common type of combined nevi (Clinical Pearl 10). The classic bicomponent pattern -- a central blue-black structureless area (the deep dermal blue nevus component) with peripheral brown pigment network (the junctional or compound nevus component) -- is characteristic. The critical dermoscopic skill is recognizing this as a combined nevus rather than melanoma with blue-white veil. In melanoma, the blue-white veil would be asymmetric and accompanied by additional melanoma-specific structures (irregular streaks, regression, atypical dots). Here, the blue-black area is homogeneous and the peripheral network is regular and symmetric, both favoring a benign diagnosis. In a young patient with a stable lesion, this pattern may be monitored. If any doubt exists, biopsy is recommended.
Clinical Scenario A 52-year-old woman with a history of cutaneous melanoma excised 3 years ago from the left upper back presents with a new 6 mm blue-black papule on the left posterior shoulder, approximately 5 cm from the previous excision scar. The lesion appeared 6 months ago. Dermoscopy reveals a blue-black structureless area that is somewhat heterogeneous, with subtle color variation from blue to blue-gray. Small irregular vessels are visible at the periphery.
What is the most likely diagnosis?
Diagnosis: Must rule out melanoma metastasis -- biopsy is mandatory.
This case illustrates two critical clinical pearls simultaneously. First, Clinical Pearl 2: a new blue lesion in an adult with a history of melanoma demands heightened suspicion and usually biopsy. Second, Clinical Pearl 6: in a patient with a history of invasive melanoma, any new blue-black lesion near a previous excision site should be evaluated as a potential melanoma metastasis until proven otherwise. The small irregular vessels at the periphery are an additional warning sign of malignancy. While this could be a new blue nevus, the clinical context -- history of melanoma, proximity to previous excision site, recent onset, heterogeneous color, and peripheral vessels -- makes metastasis a realistic concern that cannot be excluded by dermoscopy alone. Excisional biopsy is essential.
9. Cross-References
| Topic | Source Location | Page(s) |
|---|---|---|
| Blue nevi -- full chapter | Chapter 7d | 164--168 |
| Homogeneous blue pattern (overview) | Chapter 7b | 150--151 |
| Combined nevus overview | Chapter 7b | 155--156 |
| Blue-whitish veil in melanoma | Chapter 3 / Module 02 | 20--52 |
| Dermoscopy colors and depth correlation | Chapter 3 / Module 02 | 20--25 |
| Nodular melanoma (differential) | Chapter 8b | 198--200 |
| Melanoma metastasis dermoscopy | Chapter 8e / 10 | 213--253 |
| Vascular lesions (hemangioma, angiokeratoma, Kaposi) | Chapter 6f | 136--142 |
| Basal cell carcinoma -- pigmented | Chapter 6b | 108--112 |
| Dermatofibroma (hemosiderotic variant) | Chapter 6a | 101--107 |
| Spitz and Reed nevi | Chapter 7e | 180--186 |
10. Related Modules
| Module | Title | Relationship to This Module |
|---|---|---|
| Module 01 | Introduction and Principles of Dermoscopy | Prerequisite -- polarized light dermoscopy technique needed to visualize shiny white lines and other structures in blue nevi. |
| Module 02 | Histopathologic Correlations | Prerequisite -- understanding of blue color as deep dermal melanin is foundational to blue nevus recognition. |
| Module 08 | Dermatofibroma | Sclerotic blue nevi with central white areas mimic hemosiderotic dermatofibromas; comparative dermoscopy skills essential. |
| Module 09 | Basal Cell Carcinoma | Pigmented BCC with blue ovoid nests is a key differential; blue in BCC is in nests, not diffuse. |
| Module 13 | Vascular Lesions | Angiokeratoma, Kaposi sarcoma, and hemangioma can present as blue lesions. |
| Module 16 | Acquired Melanocytic Nevi | Combined nevi (blue + compound/junctional) bridge the acquired nevi and blue nevi domains. |
| Module 19 | Spitz and Reed Nevi | Pigmented Reed nevi with blue-black color enter the blue lesion differential; also combined Spitz/Reed + BN exists. |
| Module 22 | Nodular Melanoma | Primary differential diagnosis for blue lesions; nodular melanoma may show blue-black homogeneous pattern with additional warning features. |
| Module 29 | Collision Tumors and Exceptions | Combined blue nevi are a form of collision/combined tumor; understanding bicomponent patterns prevents misdiagnosis as melanoma. |
| Module 33 | Nails | Subungual blue nevus presenting as blue melanonychia requires nail-specific evaluation approaches. |
This module is part of the Dermoscopy Educational Course.
Image Sources & Citations
- DERM12345 (Skin Lesion Dataset with 40 Subclasses): DERM12345: A Large-scale Skin Lesion Image Dataset with 40 Subclasses. Figshare. 2023. License: CC-BY-4.0.
