Module 11: SCC Spectrum -- Bowen Disease, Keratoacanthoma, and Squamous Cell Carcinoma
Source: Dermoscopy Educational Course Authors: Iris Zalaudek, Alan Cameron, Cliff Rosendahl, Shushanik Karapetyan, and Pawel Pietkiewicz
1. Learning Objectives
After completing this module, the learner should be able to:
- Describe the keratinocyte carcinoma spectrum from actinic keratosis through Bowen disease, keratoacanthoma, and invasive squamous cell carcinoma, and explain how dermoscopic features evolve along this continuum.
- Identify the archetypal dermoscopic pattern of nonpigmented Bowen disease -- glomerular (coiled) vessels in a clustered or linear arrangement with surface scale -- and explain why the simultaneous finding of these two features yields a 98% diagnostic probability for Bowen disease.
- Recognize the dermoscopic features of pigmented Bowen disease, including brown or gray dots in linear radial arrangement at the periphery, eccentric pink structureless areas, and glomerular vessels, and differentiate pigmented Bowen disease from melanoma.
- Describe the characteristic dermoscopic features of keratoacanthoma, including central keratin mass, hairpin (looped) vessels with white-to-yellow background halo, linear irregular (serpentine) vessels, white circles, and white structureless areas.
- Identify the dermoscopic features of invasive SCC, including polymorphous vessels (hairpin, dotted, glomerular, linear irregular), surface keratin, white circles, white structureless areas, ulceration, and blood crusts.
- Distinguish well-differentiated from poorly differentiated SCC based on dermoscopic features such as the presence or absence of keratin clues, growth pattern (exophytic vs. endophytic), color, and vascular coverage.
- Apply the five diagnostic pillars for evaluating nonpigmented keratinizing tumors: clinical features, keratin clues, vessel morphology, vessel arrangement/distribution, and additional criteria (rosettes, strawberry pattern).
- Construct a differential diagnosis for SCC-spectrum lesions, distinguishing them from BCC, amelanotic melanoma, seborrheic keratosis, viral warts, and inflammatory conditions.
2. Prerequisites
- Module 01: Introduction and Principles of Dermoscopy -- Equipment, polarized vs. nonpolarized light, contact vs. noncontact dermoscopy
- Module 02: Histopathologic Correlations -- Keratin structures, vascular patterns, and their histologic substrates
- Module 10: Actinic Keratosis -- Strawberry pattern, follicular plugs with halo (FPWH), rosettes, AK grading, and the concept of progression from AK to SCC in situ
3. Key Concepts
The AK-to-SCC Continuum
The spectrum of premalignant and malignant keratinizing tumors comprises actinic (solar) keratosis (AK), Bowen disease (BD), keratoacanthoma (KA), and squamous cell carcinoma (SCC). These tumors may be viewed as lying on a continuum of keratinocyte dysplasia:
- AK Grade I: Atypia confined to the lower epidermis
- AK Grade II: Atypia extending to the mid-epidermis; prominent FPWH, strawberry pattern, scale
- AK Grade III (hypertrophic AK): Near-full-thickness dysplasia with prominent adherent scale-crust and structureless areas
- Bowen disease / SCC in situ: Full-thickness keratinocyte dysplasia
- Keratoacanthoma: Considered by many a well-differentiated SCC variant with rapid growth followed by spontaneous involution
- Invasive SCC: Dermal invasion, ranging from well-differentiated to poorly differentiated
Because these tumors exist on a spectrum, their clinical and dermoscopic features show considerable overlap, making strict categorical separation difficult in many cases.
Diagnostic Framework for Nonpigmented Keratinizing Tumors
The great majority of keratinizing tumors are nonpigmented, meaning their dermoscopic diagnosis relies on:
- Clinical assessment: Texture, firmness, rate of growth, presence of ulceration, surface keratin
- Keratin clues: Surface keratin, white circles, white structureless areas, four-dot clods (rosettes)
- Vascular morphology: Dotted, glomerular/coiled, hairpin/looped, linear irregular/serpentine, polymorphous
- Vessel arrangement and distribution: Clustered, linear, random, diffuse, focal
- Additional dermoscopic criteria: Rosette sign (polarized light only), strawberry pattern
Keratin clues have been shown to be more robust than vessel clues and take diagnostic priority when present. White circles in SCC/KA carry 87% specificity.
Technical Considerations
- Contact dermoscopy may compress blood vessels, rendering them invisible. Using a viscous immersion medium (ultrasound gel) permits examination without excessive pressure.
- Polarized light dermoscopy eliminates pressure-induced compression entirely, greatly improving vascular visualization.
- Vessel morphology alone is less specific than other dermoscopic structures, as the same morphology may appear in different tumor types and even in inflammatory lesions.
- On the lower limbs, dotted and coiled vessels may be seen in lesions (e.g., BCC) that elsewhere rarely show these patterns.
4. Core Content
4.1 The Keratinocyte Carcinoma Spectrum
Keratinizing tumors represent a biological continuum of progressive keratinocyte dysplasia. While dermoscopy cannot always precisely place a given lesion on the spectrum, it provides critical information through two major categories of findings:
Keratin clues (structural features reflecting the keratinization process):
- Surface keratin (white-to-yellow scale)
- White circles (correlating with dilated, keratin-filled follicular openings or concentric keratinization)
- White structureless areas (corresponding to masses of highly keratinized keratinocytes)
- Four-dot clods / rosettes (polarized light only; keratin in follicular openings/eccrine ducts)
Vascular patterns (reflecting the neovascular response and tumor architecture):
- Dotted vessels
- Glomerular (coiled) vessels
- Hairpin (looped) vessels
- Linear irregular (serpentine) vessels
- Polymorphous (combinations of two or more types)
The arrangement and distribution of vessels provide additional specificity beyond morphology alone. For example, glomerular vessels are seen in BD (clustered/linear arrangement), stasis dermatitis (random distribution), and psoriasis (regular distribution throughout the lesion).
4.2 Bowen Disease (SCC In Situ)
4.2.1 Nonpigmented Bowen Disease
BD and intraepidermal carcinoma (IEC) represent SCC in situ of the skin. Although some consider BD and IEC to be separate entities based on epidemiologic, clinical, and histopathologic features, dermoscopic differences between the two are not well defined.
Archetypal dermoscopic pattern:
- Surface scale: White-to-yellow surface scale on an erythematous to yellow background
- Glomerular (coiled) vessels: Tortuous capillaries mimicking the glomerular apparatus of the kidney, arranged in clustered or linear patterns
The simultaneous finding of surface scale and focal clusters of glomerular vessels has been reported to give a 98% diagnostic probability that the lesion is BD.
Imaging challenges: Although glomerular/coiled vessels are usually easy to see through a dermatoscope, their coiled morphology is often difficult to capture on images. Due to their small size, lack of contrast, and camera resolution limitations, these vessels often appear as red dots in photographs. This creates potential confusion with the dotted vessels of melanocytic tumors (e.g., Spitz nevi). The key differentiator is distribution:
- BD: Vessels are clustered or in linear arrangement
- Spitz nevi: Vessels are symmetrically and randomly distributed
Additional clues distinguishing BD from Spitz nevi include reticular depigmentation (negative network) in Spitz nevi and surface scale in BD.
Differential diagnosis of BD: Features may occasionally overlap with BCC, amelanotic melanoma, seborrheic keratosis, lichen planus-like keratosis, and AK.
4.2.2 Pigmented Bowen Disease
Pigmented Bowen disease (pBD) is less frequent than its nonpigmented counterpart and is more common in darker skin phenotypes. In an analysis of more than 50 consecutive cases, the following dermoscopic patterns were identified:
- Brown or gray dots: A strong diagnostic clue when arranged as linear radial lines at the periphery of the lesion
- Pink or skin-colored eccentric structureless areas: A structureless zone eccentric within the lesion
- Glomerular (coiled) vessels: Arranged randomly, as clusters, or in radial lines
Pigmented circles: Dermoscopic pigmented circles in pBD correlate on confocal microscopy with pigmented basal keratinocytes rimming the dermal papillae. The circular morphology is often only revealed at higher magnification. These may also be observed as pigmented circles in a linear arrangement.
Differentiating pBD from melanoma: pBD may occasionally mimic melanoma. Features supporting a diagnosis of pBD include:
- Adherently scaly surface
- Brown or gray dots arranged in linear radial lines at the periphery
- Focal glomerular (coiled) vessels
In contrast, melanoma typically shows:
- Brown/gray dots that do not follow a linear/radial pattern
- Dotted (red dots) or polymorphous vessel morphology (rather than glomerular)
4.2.3 Bowenoid Actinic Keratosis
Bowenoid AK reveals nearly full-thickness keratinocyte dysplasia histologically. Its dermoscopic appearance is similar to BD; however:
- Glomerular vessels tend to be regularly (uniformly) distributed rather than arranged in focal clusters as in classic BD
- The distinction between Bowenoid AK and BD is primarily histopathologic rather than dermoscopic
4.2.4 Erythroplasia of Queyrat
Erythroplasia of Queyrat (EQ) is Bowen disease of the glans penis. In a study of 14 cases compared with psoriasis, Zoon plasma cell balanitis, and candida balanitis:
- Glomerular (coiled) vessels, both clustered and randomly distributed, were highly predictive of EQ
Check Your Understanding
What dermoscopic features characterize Bowen disease (SCC in situ)?
Bowen disease is characterized by glomerular (coiled) vessels arranged in clusters, surface scale/crust, and a pink-red background. The glomerular vessels are the most specific dermoscopic clue. Additional features may include brown dots arranged in linear patterns and small hemorrhagic foci.
Clinical Scenario
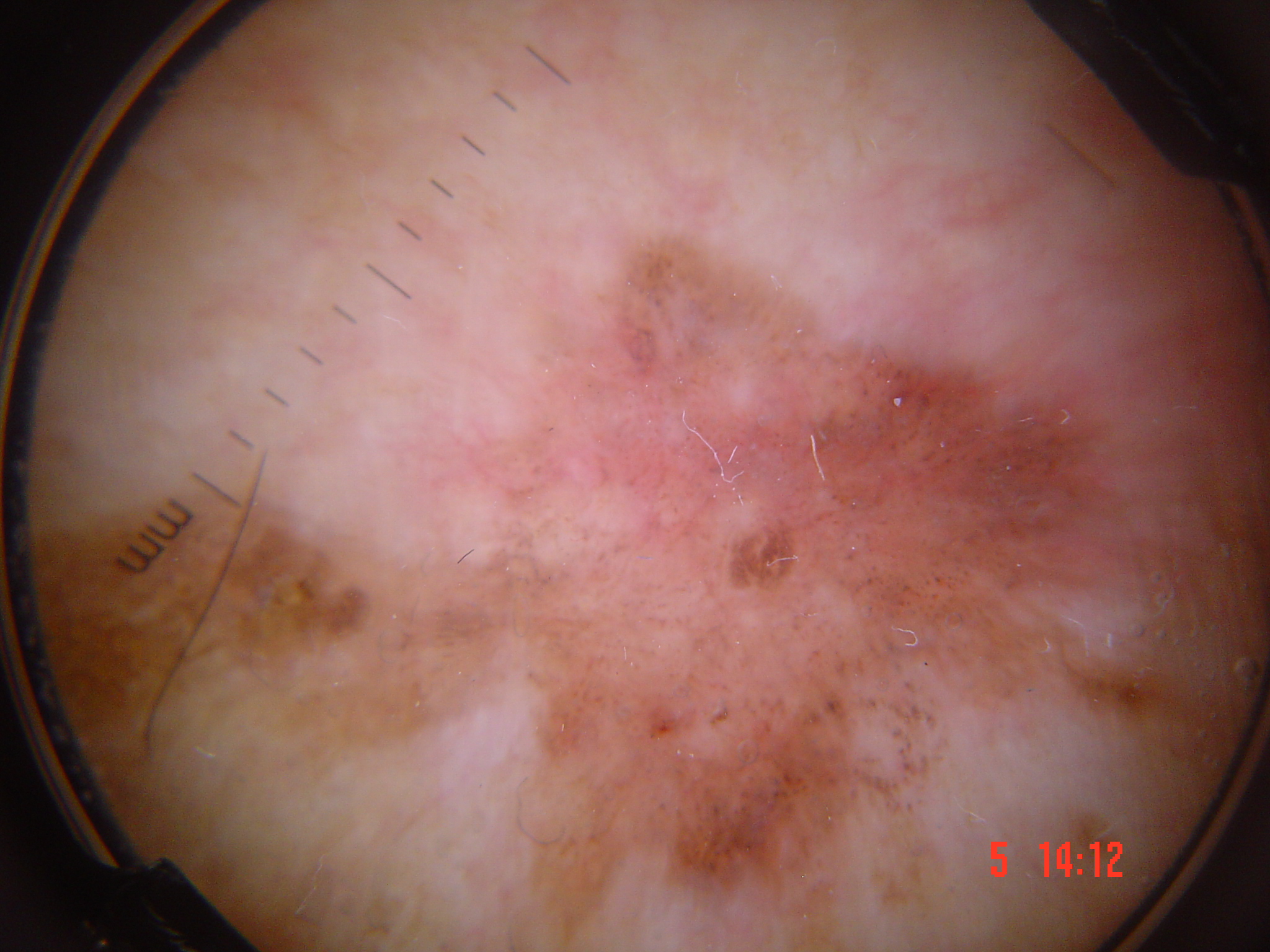
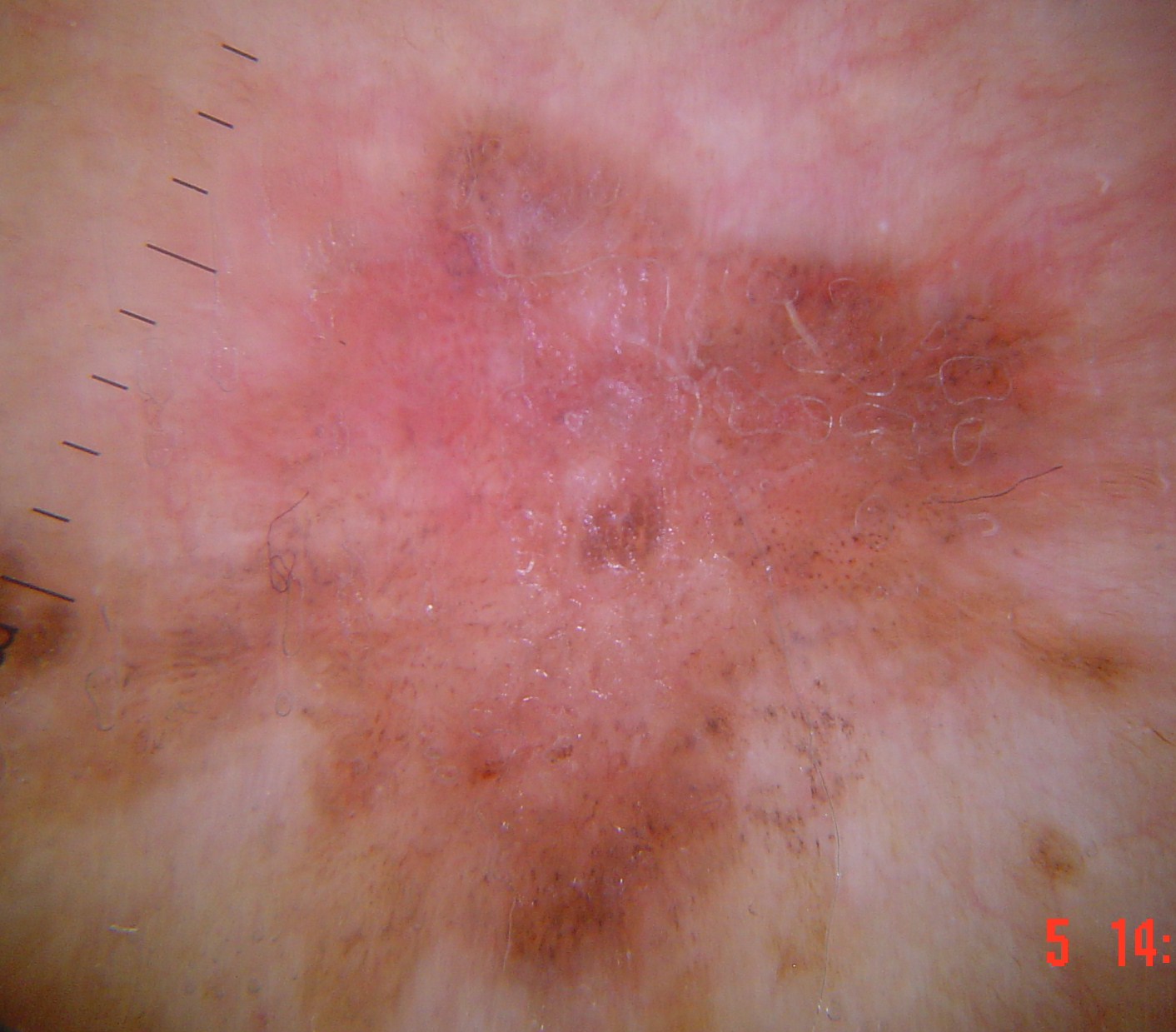
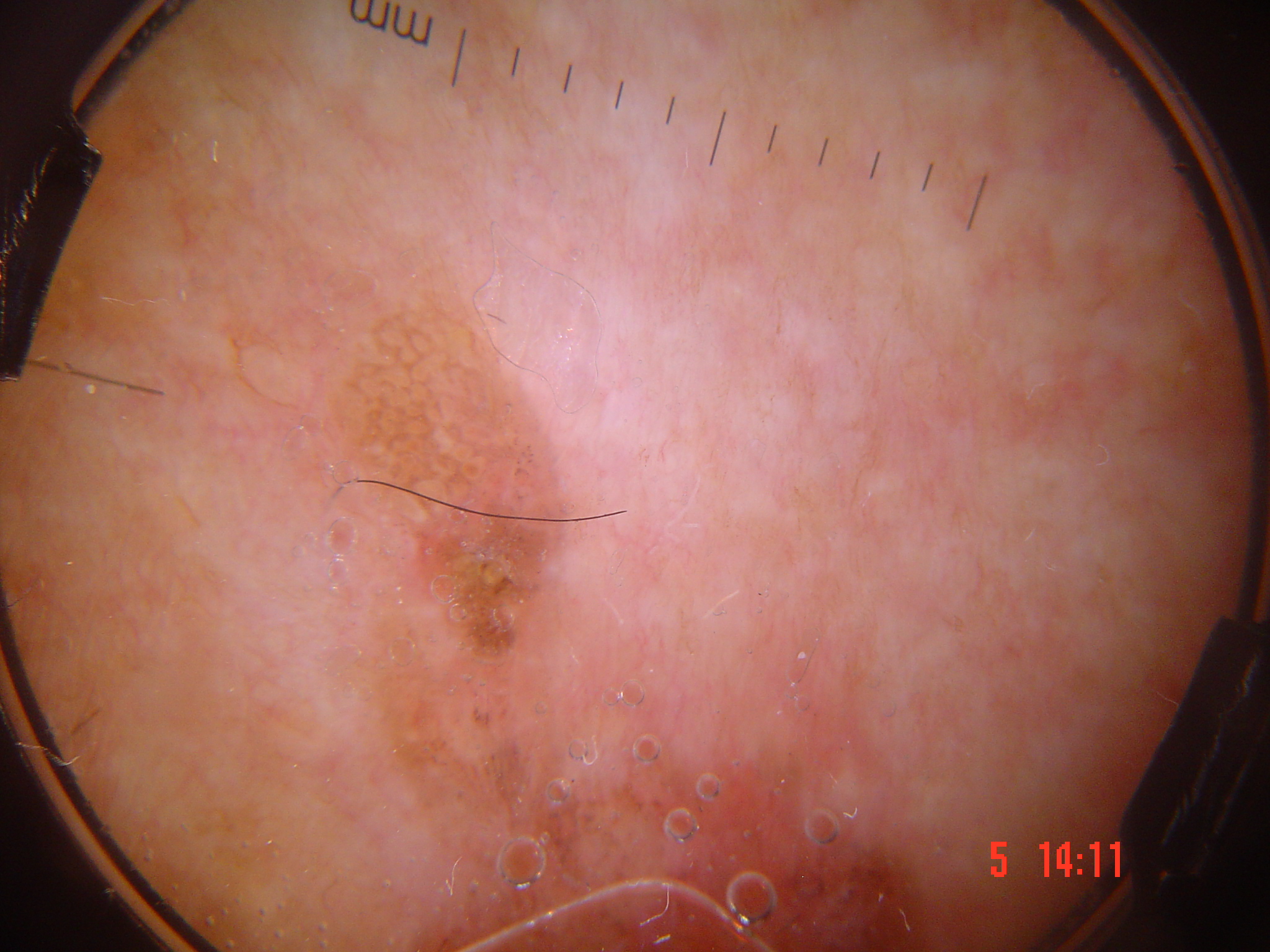
A 58-year-old woman presents with a persistent, erythematous, scaly plaque on the left lower leg that has been present for over a year. Dermoscopy reveals tightly coiled vessels (glomerular vessels) arranged in clusters distributed across the lesion surface. Brown dots and small globules are arranged in a linear fashion within the plaque. The surface shows fine scale. No white circles or hairpin vessels are identified.
What is your diagnosis and key dermoscopic findings?
Bowen disease (SCC in situ, pigmented variant)
Glomerular (coiled) vessels are the hallmark dermoscopic vascular feature of Bowen disease, corresponding to tightly coiled capillaries within the elongated dermal papillae of the acanthotic epidermis. The clustered distribution distinguishes them from the randomly scattered dots of melanoma. The linearly arranged brown dots and globules indicate pigmented Bowen disease, where aggregates of atypical basal pigmented keratinocytes create these structures. This pigmented variant can mimic melanoma, but the characteristic glomerular vessels and linear arrangement of pigmented structures support the diagnosis of Bowen disease.
Key Takeaways
- SCC in situ (Bowen disease) is characterized by glomerular vessels (coiled vessels resembling renal glomeruli) arranged in clusters, corresponding to dilated tortuous capillaries in dermal papillae.
- White circles (targetoid hair follicles) seen under polarized dermoscopy represent keratinizing concentric rings around follicular ostia and are a clue to keratinizing malignancy.
- Surface scale and keratin are prominent features of the SCC spectrum; thick yellow-white keratin masses suggest invasive SCC rather than in situ disease.
4.3 Keratoacanthoma
KA is considered by many to be a well-differentiated variant of SCC, with a typical clinical course of initial rapid growth followed by spontaneous involution over a period of a few months. Others consider it a distinct benign tumor, but this controversy does not affect dermoscopy findings.
Dermoscopic features:
KA exhibits the same keratin clues and vessel patterns as invasive SCC:
- Central keratin mass: A central yellowish to brownish structureless mass of keratin is the hallmark feature
- Keratin clues: Surface keratin, white circles, and white structureless areas are usually present. These clues are more robust than vessel clues and take diagnostic priority
- Vessels surrounding the central keratin:
- Hairpin (looped) vessels: Often with a white-to-yellow background halo -- the hallmark vascular pattern
- Linear irregular (serpentine or branched serpentine) vessels: Elongated and sometimes thick telangiectasias
- Glomerular (coiled) vessels: May also be seen
- Dotted (red dot) vessels: Occasionally present
- White structureless areas: Corresponding histologically to masses of highly keratinized keratinocytes
- White circles: Compelling clues to SCC/KA; these take priority over vessel clues
Important limitation: KA cannot reliably be distinguished from SCC dermatoscopically. Any lesion with KA features should be managed as a potential SCC.
4.4 Invasive Squamous Cell Carcinoma
Invasive SCC is usually clinically straightforward -- a firm, tender, growing nodule. Pigmented variants are exceedingly rare. The differential diagnosis is wide, comprising the full range of pink and skin-colored nodules.
4.4.1 Nonpigmented Invasive SCC
Dermoscopic features:
Vascular patterns:
- Hairpin (looped) vessels: Often surrounded by a whitish background halo
- Dotted vessels
- Glomerular (coiled) vessels
- Linear irregular (serpentine) vessels
- Polymorphous pattern: Combinations of two or more vascular morphologies; the most frequent combination is linear irregular + dotted vessels
Keratin clues:
- Surface keratin: White-to-yellow scale
- White circles: 87% specificity for SCC/KA in a study of raised nonpigmented lesions
- White structureless areas: Corresponding to keratinized cell masses
Other features:
- Ulceration and blood crusts: Irregularly distributed reddish-orange to brownish to black blotches on the tumor surface
- Rosette sign: May be present (particularly in SCC arising from AK)
- Strawberry pattern: The AK pattern of white circles on a pink/red background may be seen adjacent to and contiguous with some SCCs when SCC arises in association with AK
4.4.2 Well-Differentiated vs. Poorly Differentiated SCC
Well-differentiated (KA-type) and poorly differentiated (desmoplastic-type) SCCs have distinct clinical and dermoscopic profiles:
| Feature | Well/Moderately Differentiated | Poorly Differentiated |
|---|---|---|
| Growth pattern | Exophytic | Endophytic |
| Keratin clues | Present (scales, white circles, white structureless areas) | Absent or minimal |
| Predominant color | White and white-yellow | Red |
| Vascular features | Specific patterns (hairpin, glomerular) | Nonspecific (>50% surface covered by vessels, diffuse distribution, higher vessel caliber) |
| Hemorrhages/bleeding | Less common | Frequently present |
Poor differentiation in SCC is frequently associated with:
- Endophytic growth
- No keratin clues
- Predominant red color
- More than 50% of the tumor surface covered by vessels
- Diffuse vessel distribution
- Higher vessel caliber
- Presence of hemorrhages/bleeding
Well-differentiated tumors frequently show:
- Exophytic growth
- Prominent scales and keratin clues
- Predominant white and white-yellow color
4.4.3 Pigmented Invasive SCC
Pigmented invasive SCC is rare and reveals dermatoscopically:
- Diffuse, homogeneous blue pigmentation
- Distinct, irregularly distributed blue-gray interfollicular pigment
- Dark brown to black crusts (if ulcerated)
- Vessels are usually not visible due to the pigmentation
The differential diagnosis includes pigmented BCC and melanoma.
Invasive SCC arising in pigmented Bowen disease may show dermoscopic features of pBD (brown/gray dots in linear arrangement, glomerular vessels).
4.4.4 SCC on Different Body Sites
Facial SCC: Often arises in association with AK, so the AK pattern of white circles on a pink/red background (strawberry pattern) may be seen adjacent to the SCC component. Elongated hairpin (looped) vessels are seen in the SCC, while the adjacent skin showing white circles represents the actinic keratosis component.
Nonfacial skin: Features tend to be less specific; surface scale and keratin may be the predominant findings with occasional dotted vessels.
Lower limbs: Special caution is needed -- dot and coiled vessels may be seen in lesions (such as BCC) that elsewhere only rarely show these patterns. This reduced specificity of vascular patterns on the lower extremities is an important diagnostic pitfall.
Glans penis (Erythroplasia of Queyrat): Glomerular vessels (clustered and random) are highly predictive of SCC in situ at this site.
Check Your Understanding
What is the dermoscopic hallmark of invasive SCC, and how does the vascular pattern differ from SCC in situ?
Invasive SCC typically shows a central white structureless area (representing keratinization/fibrosis), blood spots/hemorrhage, and white circles around hair follicles. The vascular pattern shifts from glomerular vessels (SCC in situ) to hairpin/looped vessels and linear irregular vessels in invasive SCC. Polymorphous vessels may also be present.
Clinical Scenario
A 81-year-old man presents with a rapidly growing, dome-shaped nodule on the dorsal hand that appeared 3 weeks ago. The lesion has a central crater filled with keratin. Dermoscopy reveals a central yellowish-brown keratin mass, bright white circles surrounding keratin plugs, white structureless areas, and hairpin (looped) vessels with a white-to-yellow background halo arranged at the periphery.
What is your diagnosis and key dermoscopic findings?
Keratoacanthoma (well-differentiated SCC variant)
The central keratin mass is the hallmark dermoscopic feature of KA, corresponding to the crateriform architecture. White circles (87% specificity for SCC/KA) correspond to acanthosis and hypergranulosis of the infundibular epidermis. White structureless areas correspond to masses of highly keratinized keratinocytes. Hairpin vessels with a white-to-yellow background halo are the hallmark vascular pattern, created by capillary loops in distorted dermal papillae, with the white halo reflecting keratinized rete ridges. The keratin clues take diagnostic priority over vessel patterns. Importantly, KA cannot be reliably distinguished from invasive SCC by dermoscopy, so this lesion should be managed as a potential SCC.
Key Takeaways
- Invasive SCC shows polymorphous vessels, white structureless areas, and central keratin/ulceration; vessel heterogeneity increases with tumor thickness and invasion depth.
- Keratoacanthoma presents with a central keratin plug, hairpin vessels with white halos at the periphery, and a symmetric architecture that helps distinguish it from conventional SCC.
- Blood spots (hemorrhagic dots due to fragile tumor vessels) are a subtle but important clue to SCC that may be seen in both in situ and invasive forms.
4.5 Differential Diagnosis
SCC vs. Basal Cell Carcinoma
- BCC characteristically shows arborizing (branching tree-like) vessels, blue-gray ovoid nests, leaf-like areas, spoke-wheel structures, and ulceration
- SCC shows keratin clues (surface keratin, white circles, white structureless areas) and polymorphous vessels
- On the lower limbs, BCC may show atypical dot and coiled vessels, creating overlap with SCC patterns
SCC vs. Amelanotic Melanoma
- Amelanotic melanoma shows polymorphous vessels (including milky-red globules/areas) and shiny white structures
- SCC has prominent keratin clues that are absent in melanoma
- The strawberry pattern (white circles on red background) is a strong indicator of AK/SCC, not melanoma
- Melanoma may have focal scale/crust, but it will not encompass the entire surface and will not become as hyperkeratotic as AK/SCC
SCC vs. Viral Wart
- Warts show the "frog spawn" pattern with thrombosed capillaries arranged in a regular dot pattern
- SCC shows polymorphous vessels in irregular distribution with keratin clues
SCC vs. Hypertrophic AK
- The transition from Grade III (hypertrophic) AK to SCC in situ represents a histologic continuum
- Dermoscopically, the transition may be marked by the appearance of glomerular vessels in clustered arrangement (suggesting BD) or polymorphous vessels (suggesting invasive SCC)
- Large areas covered by scale-crust obscuring follicular openings suggest progression from AK toward SCC
Pigmented SCC vs. Pigmented BCC and Melanoma
- Pigmented SCC shows diffuse homogeneous blue pigmentation with irregular blue-gray interfollicular pigment
- Pigmented BCC shows blue-gray ovoid nests and leaf-like areas
- Melanoma shows atypical network, irregular dots/globules, regression structures
BD vs. Inflammatory Conditions (Psoriasis, Stasis Dermatitis)
- All may contain glomerular (coiled) vessels
- BD: Vessels in clustered or linear arrangement
- Dermatoses: Vessels regularly distributed throughout the lesion (random arrangement)
- BD has adherent surface scale; psoriasis has loosely adherent silvery scale
4.6 Dermoscopic Predictors of Invasiveness and Metastatic Potential
Several dermoscopic features correlate with higher-risk SCC:
- Absence of keratin clues: Poorly differentiated SCCs frequently lack surface keratin, white circles, and white structureless areas
- Predominant red color: Indicates poor differentiation
- Endophytic growth pattern: Associated with deeper invasion
- High vascular surface coverage: More than 50% of the tumor surface covered by vessels suggests poor differentiation
- Diffuse (non-focal) vessel distribution: Non-patterned, diffuse vascularity is a marker of poor differentiation
- Higher vessel caliber: Larger-caliber vessels suggest more aggressive tumors
- Hemorrhages and bleeding: Presence of hemorrhagic foci/blood crusts as irregularly distributed reddish-orange to brownish-black blotches
- Ulceration: While present in various skin cancers, extensive ulceration in the context of a keratinizing tumor raises concern for invasive disease
- Polymorphous vessels without keratin context: When polymorphous vessels dominate without accompanying keratin clues, this suggests poorly differentiated or more aggressive disease
Check Your Understanding
What dermoscopic clue helps differentiate keratoacanthoma from conventional SCC?
Keratoacanthoma characteristically shows a central keratinous plug with a radial arrangement of hairpin (looped) vessels at the periphery, often surrounded by a white halo. The vessels radiate from the center outward. While overlap with SCC exists, the central keratin crater and radial vascular arrangement are more suggestive of keratoacanthoma.
Key Takeaways
- The SCC spectrum must be differentiated from AK (earlier stage), viral warts (frog-spawn vessels), irritated SK (similar surface features), and amelanotic melanoma (polymorphous vessels).
- Dermoscopic features progress along the AK-SCC continuum: scale and rosettes (AK) to glomerular vessels and white circles (Bowen) to polymorphous vessels and keratin masses (invasive SCC).
- Any growing keratinizing lesion with vascular polymorphism and white structureless areas that cannot be confidently diagnosed should be biopsied.
5. SCC Spectrum Features Comparison Table
| Feature | Actinic Keratosis | Bowen Disease (SCC in situ) | Keratoacanthoma | Invasive SCC (well-diff.) | Invasive SCC (poorly-diff.) |
|---|---|---|---|---|---|
| Surface scale | White-to-yellow; roughness on palpation | White-to-yellow on erythematous/yellow background | Central yellowish-brownish keratin mass | Surface keratin present | Usually absent |
| White circles | Prominent (strawberry pattern); keratin-filled follicular openings with white halo | Less prominent | Present, compelling clue | Present, 87% specificity | Usually absent |
| White structureless areas | Scale-crust in Grade III | Less common | Present (keratinized cell mass) | Present | Usually absent |
| Rosettes | Present (polarized light) | May be present | Not typically described | May be present (AK-associated SCC) | Not typically present |
| Predominant vessel type | Linear wavy, dotted (higher grades) | Glomerular (coiled) | Hairpin (looped), linear irregular (serpentine) | Polymorphous | Nonspecific, high caliber |
| Vessel arrangement | Around follicles; random | Clustered or linear | Surrounding central keratin | Variable; focal or diffuse | Diffuse (>50% surface) |
| White/yellow halo around vessels | Around follicular openings | Not prominent | Prominent white-to-yellow halo | Whitish halo may be present | Less prominent |
| Ulceration | Rare | Uncommon | Uncommon | May be present | Frequently present |
| Blood crusts / hemorrhage | Rare | Rare | Rare | May be present | Frequently present |
| Growth pattern | Flat (macule/patch) | Flat (patch/plaque) | Exophytic (dome/crater) | Exophytic (nodule) | Endophytic |
| Predominant color | Pink-red with white | Erythematous/yellow | White-yellow with peripheral vessels | White, white-yellow | Red |
| Pigmented variant features | Angulated lines, annular-granular pattern, polygons | Brown/gray dots in linear radial lines; eccentric pink areas; glomerular vessels | Not typically pigmented | Diffuse homogeneous blue; blue-gray interfollicular pigment | Rarely pigmented |
6. Vessel Pattern Comparison Table
| Vessel Type | Synonyms (Argenziano 2004 / Revised Pattern Analysis) | Morphologic Description | Tumor Associations | Key Distinguishing Features |
|---|---|---|---|---|
| Dotted | Dots | Tiny red dots densely aligned; no length or breadth | AK (higher grades), BD, SCC, melanoma, Spitz nevi | Distribution matters: clustered in BD; symmetric/random in Spitz; perifollicular in AK |
| Glomerular (coiled) | Coiled | Tortuous capillaries mimicking renal glomeruli; lines compactly convoluted | BD (archetypal), BD on glans (EQ), KA (occasional), SCC, psoriasis, stasis dermatitis | Clustered/linear in BD; random/regular in dermatoses; often appear as dots in images |
| Hairpin (looped) | Looped | Vascular loops, sometimes twisted/bending; lines with one sharp 180-degree bend (U-turn) | KA, well-differentiated SCC, seborrheic keratosis, AK (hypertrophic) | Whitish halo in keratinizing tumors; no halo in SK; elongated forms in KA/SCC |
| Linear irregular (serpentine) | Straight / Serpentine | Irregularly shaped, sized, and distributed red lines; lines without a bend or with multiple bends (snakelike) | SCC, KA, BCC (arborizing variant) | In SCC/KA: accompanied by keratin clues; in BCC: bright red, sharply focused, arborizing |
| Polymorphous | Polymorphous | Combination of two or more different vessel types | SCC (especially invasive), amelanotic melanoma | Most common combination in SCC: linear irregular + dotted; in melanoma: milky-red areas added |
| Monomorphous | Monomorphous | One vascular pattern dominates | BD (glomerular), KA (hairpin), benign lesions | Monomorphous glomerular + scale = 98% probability of BD |
| Strawberry pattern | White circles on a red background | Erythema resembling pink-red pseudonetwork around follicles; wavy vessels; keratotic plugs in white-haloed follicles | Facial AK, facial SCC arising in AK | Strong indicator of AK/SCC; not seen in melanoma; the circle is equidistant from a central point |
7. Clinical Pearls
The 98% rule: The simultaneous finding of surface scale AND focal clusters of glomerular (coiled) vessels gives a 98% diagnostic probability of Bowen disease. This is the single most powerful dermoscopic combination in the SCC spectrum.
Keratin clues trump vessel clues: In raised nonpigmented lesions, the keratin clues of surface keratin, white circles, and white structureless areas are more diagnostically robust than vascular patterns. When keratin clues and vessel clues are both present, prioritize the keratin findings.
KA and SCC are dermoscopic twins: Keratoacanthoma cannot reliably be distinguished from invasive SCC by dermoscopy alone. Always manage a lesion with KA features as a potential SCC, regardless of the clinical impression of involution.
Image artifacts with glomerular vessels: Coiled vessels in BD often appear as simple red dots in photographs due to small size and limited resolution. Look for the clustered distribution pattern to avoid confusing them with the dotted vessels of melanocytic tumors (Spitz nevi).
Vessel distribution is the differentiator: When the same vessel morphology appears in multiple conditions, arrangement is key. Glomerular vessels that are clustered or in linear arrangement suggest BD; the same vessels regularly distributed throughout suggest an inflammatory condition (psoriasis, dermatitis).
Lower limb caution: On the lower limbs, dot and coiled vessels may appear in BCC and other lesions that elsewhere rarely show these patterns. Do not rely solely on vessel morphology for diagnosis on the lower extremities.
The white halo sign: Hairpin (looped) vessels surrounded by a whitish halo are characteristic of all keratinizing tumors (benign and malignant). The absence of this halo around hairpin vessels should prompt consideration of non-keratinizing diagnoses.
Poorly differentiated SCC -- the "red flag" pattern: When you see a nodule that is predominantly red with high vascular coverage (>50% surface), diffuse vessel distribution, high-caliber vessels, hemorrhage, and NO keratin clues -- think poorly differentiated SCC. This pattern carries the highest risk.
The AK-SCC transition zone: SCC arising in AK often shows a recognizable transition -- white circles on a pink/red background (the AK component) adjacent to the SCC component with elongated hairpin vessels. Recognizing this transition can help identify early invasive disease.
Pigmented BD imitating melanoma: When a pigmented lesion shows surface scale, brown/gray dots arranged in linear radial lines at the periphery, and focal glomerular vessels -- suspect pBD rather than melanoma. The linear radial arrangement of dots is the key distinguishing feature.
Polarized light advantage: Use polarized light dermoscopy when evaluating keratinizing tumors. It eliminates pressure-induced vessel compression and enables visualization of rosettes (four-dot clods), which cannot be seen with nonpolarized dermoscopy.
Palpation still matters: In pigmented lesions on the face, the distinction between pigmented AK and lentigo maligna may ultimately require touch. Pigmented AK has a rough texture; lentigo maligna is smooth.
Clinical Vignettes
Clinical Scenario A 72-year-old man presents with a 15 mm persistent, well-demarcated, erythematous, scaly plaque on the right shin that has been present for over a year. Dermoscopy reveals white-to-yellow surface scale overlying an erythematous background. Within the lesion, tightly coiled (glomerular) vessels are arranged in distinct focal clusters. No hairpin vessels, white structureless areas, or hemorrhage is seen.
What is the most likely diagnosis?
Diagnosis: Bowen disease (squamous cell carcinoma in situ).
This is a textbook presentation of Bowen disease demonstrating the "98% rule": the simultaneous finding of surface scale AND focal clusters of glomerular (coiled) vessels gives a 98% diagnostic probability of BD. The clustered arrangement of glomerular vessels is key -- this same vessel type in a regularly distributed pattern would suggest psoriasis or dermatitis instead. The lower limb location is classic for Bowen disease. The absence of hairpin vessels with white halo argues against well-differentiated SCC, and the monomorphous vascular pattern (glomerular only) further supports BD over invasive SCC.
Clinical Scenario A 65-year-old woman presents with a rapidly growing 18 mm dome-shaped nodule on the dorsal hand that appeared 6 weeks ago. There is a central keratinous crater. Dermoscopy shows a radial arrangement of hairpin (looped) vessels with white halos converging toward the center. White circles are visible, and a central keratin mass is surrounded by a white structureless rim. No glomerular vessels, hemorrhage, or ulceration is present.
What is the most likely diagnosis?
Diagnosis: Keratoacanthoma -- but must be managed as potential SCC.
The rapid growth, central keratin crater, radially arranged hairpin vessels with white halos, and white circles all point toward keratoacanthoma. However, this case illustrates Clinical Pearl 3: KA and SCC are dermoscopic twins. Keratoacanthoma cannot reliably be distinguished from well-differentiated invasive SCC by dermoscopy alone. Despite the classic clinical history of rapid growth and the typical dermoscopic pattern, excisional biopsy (not shave) is mandatory to evaluate the full architecture and rule out invasive SCC. A shave biopsy would be inadequate to assess depth of invasion.
Clinical Scenario A 78-year-old man presents with a 22 mm erythematous nodule on the left temple. The lesion is firm, indurated, and has been growing for 3 months. Dermoscopy reveals polymorphous vessels including linear irregular vessels combined with dotted vessels. The vascular pattern covers more than 50% of the lesion surface. There is focal hemorrhage, no surface keratin, and no white structureless areas. A subtle white shiny area is visible with polarized dermoscopy.
What is the most likely diagnosis?
Diagnosis: Poorly differentiated invasive squamous cell carcinoma.
This case demonstrates the "red flag" pattern of poorly differentiated SCC (Clinical Pearl 8): a nodule that is predominantly red with high vascular coverage (>50%), diffuse vessel distribution, high-caliber linear irregular vessels combined with dotted vessels (polymorphous pattern), hemorrhage, and crucially NO keratin clues. The absence of surface keratin, white circles, and white structureless areas indicates the tumor has lost its keratinizing capacity -- a hallmark of poor differentiation. The white shiny area (chrysalis/crystalline structures) under polarized light is consistent with stromal invasion. This pattern carries the highest risk and warrants urgent excision with appropriate margins. The polymorphous vascular pattern also raises amelanotic melanoma in the differential, making histological confirmation critical.
9. Cross-References
| Topic | Reference |
|---|---|
| Chapter 6d full text | pp. 108--115 |
| Vessel morphology definitions | p. 109 |
| Nonpigmented AK (strawberry pattern, rosettes) | pp. 109--110;--6d.4 |
| Pigmented AK vs. lentigo maligna | pp. 110--111;--6d.7 |
| Nonpigmented Bowen disease | pp. 110--111;--6d.11 |
| Pigmented Bowen disease | pp. 111--112;--6d.14 |
| Bowenoid actinic keratosis | p. 112; |
| Erythroplasia of Queyrat | p. 112; |
| Keratoacanthoma | pp. 112--113;--6d.18 |
| Invasive SCC (nonpigmented) | pp. 112--114;--6d.22 |
| Well vs. poorly differentiated SCC | pp. 113--114 |
| Pigmented invasive SCC | p. 114; |
| Key points summary | pp. 114--115 |
| Chapter 6c: Actinic Keratosis (standalone) | pp. 102--107 |
| AK dermoscopic features and grading | pp. 102--106;--6c.10 |
Key References from the Chapter
- Argenziano, G, et al. Vascular structures in skin tumors: a dermoscopy study. Arch Dermatol. 2004;140:1485--9.
- Cameron, A, et al. Dermatoscopy of pigmented Bowen's disease. J Am Acad Dermatol. 2010;62:597--604.
- Lallas, A, et al. The clinical and dermoscopic features of invasive cutaneous SCC depend on the histopathological grade of differentiation. Br J Dermatol. 2015;172:1308--15.
- Pan, Y, et al. Dermatoscopy aids in the diagnosis of the solitary red scaly patch or plaque. J Am Acad Dermatol. 2008;59:268--74.
- Rosendahl, C, et al. Dermoscopy of squamous cell carcinoma and keratoacanthoma. Arch Dermatol. 2012;148:1386--92.
- Zalaudek, I, et al. Dermatoscopy of facial actinic keratosis, intraepidermal carcinoma, and invasive squamous cell carcinoma: a progression model. J Am Acad Dermatol. 2012;66:589--97.
10. Related Modules
| Module | Relationship |
|---|---|
| Module 01: Introduction and Principles of Dermoscopy | Prerequisite -- polarized vs. nonpolarized light, equipment for vascular visualization |
| Module 02: Histopathologic Correlations | Prerequisite -- histologic substrates of keratin structures and vascular patterns |
| Module 05: Prediction without Pigment | Complementary -- decision algorithm for nonpigmented lesions; vessel analysis framework |
| Module 06: Chaos and Clues Triage Algorithm | Complementary -- triage approach applicable to SCC-spectrum lesions |
| Module 09: Basal Cell Carcinoma | Differential diagnosis -- BCC vs. SCC distinguishing features |
| Module 10: Actinic Keratosis | Direct prerequisite -- AK grading, strawberry pattern, the AK-to-SCC continuum |
| Module 12: Solar Lentigines, Seborrheic Keratoses, and LPLK | Differential diagnosis -- SK features (hairpin vessels without white halo, milia-like cysts) vs. SCC features |
| Module 23: Lentigo Maligna | Differential diagnosis -- pAK vs. LM; pigmented SCC differential |
| Module 26: Amelanotic and Hypomelanotic Melanoma | Differential diagnosis -- amelanotic melanoma vs. SCC vascular patterns |
| Module 30: Face | Site-specific application -- facial AK/SCC patterns, strawberry pattern, pseudonetwork |
| Module 36: Inflammoscopy | Differential diagnosis -- distinguishing BD vessels from psoriasis and stasis dermatitis |
Image Sources & Citations
- DERM12345 (Skin Lesion Dataset with 40 Subclasses): DERM12345: A Large-scale Skin Lesion Image Dataset with 40 Subclasses. Figshare. 2023. License: CC-BY-4.0.