Module 08: Nonmelanocytic Lesions -- Dermatofibroma
Source: Atlas of Dermoscopy, 3rd Edition -- Chapter 6a (pp. 90--96) Authors: Silvia E. Mancebo and Michael A. Marchetti
1. Learning Objectives
After completing this module, the learner should be able to:
- Define dermatofibroma and describe its clinical presentation, including the classic dimple (Fitzpatrick) sign.
- Identify the most common dermoscopic pattern of dermatofibroma: a delicate peripheral pigment network surrounding a central white structureless patch.
- Recognize all 10 classified dermoscopic patterns of dermatofibroma and associate each with its approximate prevalence.
- Distinguish features seen with polarized versus nonpolarized dermoscopy and contact versus noncontact techniques as applied to dermatofibroma.
- Describe the dermoscopic and histopathologic features of dermatofibroma variants, including aneurysmal/hemosiderotic, atrophic, lipidized, and seborrheic keratosis-like types.
- Explain the histopathologic correlates of key dermoscopic structures in dermatofibroma (pigment network, central white patch, ring-like globules, shiny white structures).
- Differentiate dermatofibroma from its primary mimickers (melanoma, Spitz nevus, basal cell carcinoma, and dermatofibrosarcoma protuberans) using clinical and dermoscopic criteria.
- Identify features of dermatofibroma that warrant histopathologic evaluation for diagnostic confirmation.
2. Prerequisites
- Module 01: Introduction and Principles of Dermoscopy -- understanding of polarized versus nonpolarized dermoscopy, contact versus noncontact technique
- Module 02: Histopathologic Correlations of Dermoscopic Structures -- familiarity with pigment network formation, structureless areas, and shiny white structures
3. Key Concepts
What Is a Dermatofibroma?
A dermatofibroma (also known as benign fibrous histiocytoma) is a benign proliferation of fibrohistiocytic cells that may occur anywhere on the skin surface but has a predilection for the extremities of adults. These tumors are among the most commonly encountered benign skin lesions in dermatology.
Clinical Context
- Presentation: Single or multiple, round to ovoid, firm papules, plaques, or nodules
- Size: Usually less than 1 cm in diameter
- Color: Variable -- light to dark brown, purple, or red
- Dimple (Fitzpatrick) sign: Characteristic dimpling of the tumor upon lateral compression; this clinical sign is a hallmark of dermatofibroma and aids bedside diagnosis
- Histologic variants: Multiple clinical and histologic variants exist, each producing different dermoscopic features
- Key differential: Must be differentiated from melanoma, basal cell carcinoma, squamous cell carcinoma, and melanocytic nevi
Why Dermoscopy Matters
Although most dermatofibromas can be reliably identified as benign tumors after clinical and dermoscopic examination, some dermatofibromas cannot be distinguished from melanoma and therefore warrant histological evaluation for diagnostic confirmation. Understanding the full spectrum of dermoscopic patterns is essential for confident diagnosis and appropriate triage.
4. Core Content
4.1 Dermoscopy Light Source and Technique
The dermoscopic appearance of dermatofibroma varies significantly depending on the light source and technique employed. Awareness of these differences is critical for accurate interpretation.
Polarized versus Nonpolarized Dermoscopy
| Feature | Nonpolarized Dermoscopy | Polarized Dermoscopy |
|---|---|---|
| Shiny white structures | Not visualized | Visualized (shiny white blotches and streaks) |
| Blood vessels | Less apparent or absent | Accentuated appearance |
| Superficial epidermal features | Accentuated (ridges, fissures, comedo-like openings, milia-like cysts, mammillated surface) | Less conspicuous |
| Central white patch | Present | Appears brighter, may have a pink hue |
Contact versus Noncontact Dermoscopy
- Contact dermoscopy: Vasculature findings are less apparent or not visualized at all
- Noncontact dermoscopy: Vessels are more conspicuous, vascular blush and dotted vessels become prominent
The physical and optical properties underlying these differences are detailed in Module 01 (see also textbook Chapter 2).
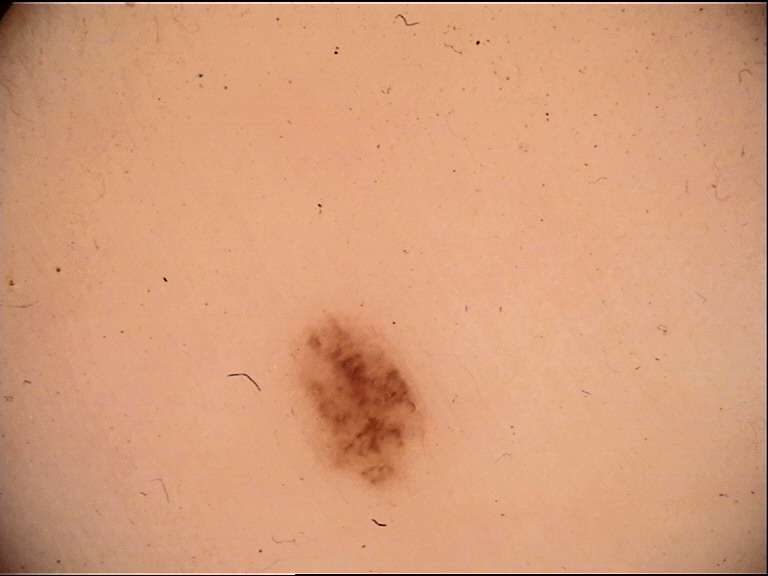
4.2 Classic Dermoscopic Pattern
The classically described presentation using nonpolarized dermoscopy consists of:
- Central structureless white patch (previously termed "scar-like area")
- Delicate peripheral pigment network surrounding the central patch
This is the most common pattern overall (Pattern 2 in Table 6a.1, prevalence 35%).
Histopathologic Correlates
| Dermoscopic Structure | Histopathologic Correlate |
|---|---|
| Pigment network | Hyperpigmentation of basal layer keratinocytes situated along elongated rete ridges |
| Central structureless white patch | Attenuated epidermis overlying a fibrous histiocytic stroma in the papillary dermis |
| Ring-like globules | Widely spaced, flattened and broad hyperpigmented rete ridges surrounded by an attenuated epidermis |
Check Your Understanding
What is the classic dermoscopic pattern of dermatofibroma under nonpolarized dermoscopy?
The classic pattern consists of a central structureless white patch (previously termed 'scar-like area') surrounded by a delicate peripheral pigment network. This combination is present in approximately 70% of dermatofibromas.
4.3 Pigment Network
The pigment network in dermatofibroma has specific qualitative characteristics:
- Composition: Thin, light to dark brown lines
- Quality: Characteristically fine or lacey
- Periphery: Fades gradually into the surrounding normal skin
- Center-ward transition: Toward the center of the lesion, the network may cease to look reticulated and instead may resemble "ring-like" globular or clod-like structures
Prevalence Data (Zaballos et al., n = 412)
- Pigment network present in 72% of dermatofibromas
- Majority displayed a typical delicate pigment network
- 3% had an atypical or broadened pigment network
- Location of pigment network:
- Periphery of lesion: 71%
- Throughout the lesion: 27%
- Irregularly distributed: 3%
Important: When the pigment network is atypical or irregularly distributed, excision with histopathologic confirmation is recommended.
Structureless Pigmentation
- Present in 25% of dermatofibromas
- Distribution:
- Periphery: 55%
- Throughout the entire lesion: 24%
- Center of lesion: 24%
- Irregularly and multifocally distributed: 3%
- Color: Most often brown; occasionally bluish or reddish-bluish colors observed
4.4 Central White Structureless Patch
This is the second most common individual feature in dermatofibromas.
- Present in 57% of 412 dermatofibromas (Zaballos et al.)
- Most common presentation: single, well-demarcated patch located in the lesional center
- Less common variants:
- Multiple white scar-like patches: 12%
- Distributed throughout the lesion: 10%
- Irregularly distributed: 3%
Key Takeaways
- The classic dermatofibroma pattern is a delicate peripheral pigment network surrounding a central white structureless patch, seen in 35% of cases.
- The pigment network in dermatofibroma is characteristically fine, lacey, and fades gradually into surrounding skin, present in 72% of cases.
- The central white patch has a histopathologic correlate of attenuated epidermis overlying fibrous stroma and is present in 57% of dermatofibromas.
4.5 Ring-Like Globules and the "White Network"
Ring-like globules are a distinctive feature of dermatofibroma:
- Characteristically round or oval structures
- The periphery is relatively darker than the center
- Correspond to widely spaced, flattened, and broad hyperpigmented rete ridges
- Typically found toward the center of the lesion, at the transition zone between the pigment network and the central white patch
The "White Network" Phenomenon
- Early descriptions noted a "white network" in dermatofibromas
- This is created when ring-like globules or small islands of pigmented rete ridges are surrounded by collagen (i.e., white structureless scar-like patch, shiny white structures)
- Diagnostic pitfall: This white network appearance can sometimes be difficult to differentiate from a negative network found in melanocytic tumors
4.6 Crystalline Structures (Shiny White Lines, Blotches, and Streaks)
Visible exclusively under polarized dermoscopy:
- Shiny white streaks and blotches are frequently observed within the central white patch
- Under polarized light, the central white patch appears brighter, may acquire a pink hue, and reveals these shiny structures
- Correspond to dense collagen fibers in the papillary dermis
Check Your Understanding
Why are shiny white structures (crystalline structures) visible in dermatofibroma only under polarized dermoscopy?
Shiny white structures are caused by birefringence of collagen fibers. Birefringence is a property where certain structures rotate the plane of polarized light. Since this optical phenomenon requires polarized light to be detected, these structures are completely invisible under nonpolarized dermoscopy.
Clinical Scenario
A 33-year-old woman presents with a 6 mm firm brown papule on the right lower leg that has been stable for 2 years. Lateral compression produces a dimpling of the overlying skin. Dermoscopy with nonpolarized light reveals a central structureless white patch surrounded by a delicate, lacey pigment network that fades gradually into the surrounding normal skin. At the transition zone between the network and the central white area, you observe ring-like globular structures.
What is your diagnosis and key dermoscopic findings?
Dermatofibroma (classic pattern)
This is the most common dermoscopic pattern of dermatofibroma (Pattern 2, prevalence 35%). The central structureless white patch corresponds to attenuated epidermis overlying a fibrous histiocytic stroma in the papillary dermis. The delicate peripheral pigment network corresponds to hyperpigmentation of basal keratinocytes along elongated rete ridges. The ring-like globules at the transition zone represent widely spaced, flattened, broad hyperpigmented rete ridges. The positive dimple (Fitzpatrick) sign on lateral compression provides strong clinical confirmation. The gradual fading of the network into normal skin is characteristic of dermatofibroma.
4.7 Vascular Patterns
Dermatofibromas can display a variety of vascular patterns, none of which are specific to the diagnosis:
- Vessel morphologies: Dotted, comma, hairpin, glomerular, and linear vessels
- Polymorphous vessels: Multiple vessel morphologies may be present in the same lesion
- Vascular blush: Structureless erythema may be the only vascular finding
- Best visualization: Noncontact polarized dermoscopy
- Less prevalent features: Scale, ulceration/erosion, fissures, ridges, and mammillated surface
4.8 Influence of Anatomic Location
Dermoscopic patterns vary by body site:
| Location | Most Common Pattern |
|---|---|
| Chest, back, arms, legs | Delicate peripheral network with central structureless white patch |
| Face and hands | Delicate network throughout the lesion |
| Trunk (Brancaccio et al. series) | Structureless pigmentation |
| Extremities (Brancaccio et al. series) | Central white structureless patch surrounded by delicate network |
4.9 Influence of Skin Type/Color
A prospective study of 100 dermatofibromas in Fitzpatrick skin type IV--V (Kelati et al.) found:
- The classic pattern (peripheral network with central white structureless area) was the most common subtype
- However, this pattern was significantly less prevalent compared with studies examining lighter-skinned individuals
- In skin type VI: lesions show peripheral delicate network, a gray central structureless patch, and numerous darkly pigmented ring-like globules
- In skin type I (red hair): lesions may present as nonpigmented with dotted vessels and shiny white streaks, mimicking Spitz nevus or amelanotic melanoma
Key Takeaways
- Ring-like globules at the transition zone between network and central patch are distinctive for dermatofibroma and should not be confused with the negative network of melanoma.
- Shiny white structures (visible only under polarized dermoscopy) appear within the central white patch and correspond to dense collagen fibers.
- Dermoscopic patterns vary significantly with skin phototype: darker skin shows gray central patches and darkly pigmented globules, while very fair skin may show nonpigmented patterns mimicking amelanotic melanoma.
4.10 The Ten Classified Dermoscopic Patterns
Ten global patterns have been identified, grouped into those with and without a peripheral delicate pigment network (see Reference Table in Section 5 below for full details).
4.11 Dermatofibroma Variants
Aneurysmal / Hemosiderotic Dermatofibroma
- Histology: Uncommon but distinct variant characterized by blood-filled spaces occupying up to one-half of the lesion and abundant hemosiderin in the surrounding stroma
- Relationship: Hemosiderotic dermatofibroma is considered an earlier stage in the development of the aneurysmal dermatofibroma
- Dermoscopic features:
- Central bluish or reddish structureless area with shiny white streaks
- Delicate peripheral network with variable degrees of vascular structures
- Bluish to yellowish and red-brownish hues in the center
- Scaly surface (correlates to acanthosis or hyperkeratosis)
- Yellowish structureless areas at the periphery (correlate to hemosiderin or foamy histiocytes)
- Prominent branched (arborizing-like) vessels
- Violaceous-blue structureless areas
- Prominent polymorphous vessels
- In darker skin (Fitzpatrick IV--V): A white ring around a central ulceration has been reported; the white ring may be explained by dermal fibrosis surrounding large blood-filled spaces
- Clinical significance: These dermoscopic features are not specific; melanoma cannot be confidently ruled out. Histopathologic evaluation of suspicious tumors is recommended.
Atrophic Dermatofibroma
- Clinical: Flat, atrophic, or indented papules or plaques
- Histopathology: Reduction in dermal thickness and reduction in elastic fibers
- Dermoscopy: Patchy delicate network with multiple white structureless areas
Dermatofibroma with Seborrheic Keratosis-Like Features
- Superimposed epidermal changes including acanthosis, hyperkeratosis, papillomatosis, and keratin-filled invaginations
- Dermoscopic features:
- Ridges and fissures
- Comedo-like openings
- Milia-like cysts
- Variable degrees of peripheral network, white structureless areas, and ring-like globules
Lipidized Dermatofibroma
- Histopathology: Scattered cells with foamy cytoplasm
- Dermoscopy: Yellowish structureless pigmentation in all cases
- Of 13 cases studied: 5 had total yellowish structureless pattern, 5 had an atypical pattern, 3 had a central white patch with peripheral delicate network pattern
- May show yellow clods
Dermatofibroma with Sebaceous Induction
- Reported to display whitish or white-yellow lobules
- May feature overlying sebaceous hyperplasia
Check Your Understanding
How does an atypical dermatofibroma differ dermoscopically from the classic presentation, and why is this important?
Atypical dermatofibromas may show features that overlap with melanoma, including blue-black pigmentation, irregular streaks, and asymmetric patterns. This is important because these variants account for most dermoscopy misdiagnoses of dermatofibroma, and biopsy may be warranted when the classic central white patch and peripheral network pattern are absent.
4.12 Dimple Sign and Its Dermoscopic Correlates
The dimple (Fitzpatrick) sign -- dimpling with lateral compression -- is a clinical maneuver that aids in the diagnosis of dermatofibroma. Its relevance in dermoscopy includes:
- The sign provides clinical confidence when dermoscopic features are equivocal
- Particularly useful in nonpigmented dermatofibromas (skin type I, fair-skinned individuals) where dermoscopy may show only dotted vessels and shiny white streaks
- The presence of a dimple sign combined with additional dermatofibromas of the same morphology in the same patient strengthens the clinical diagnosis
- Does not have a direct dermoscopic structural correlate but is a complementary bedside maneuver
4.13 Multiple Dermatofibromas
- Dermatofibromas may occur as single or multiple lesions
- When multiple lesions are present in the same patient, finding consistent morphology across lesions supports the diagnosis
- Multiple dermatofibromas with the same dermoscopic pattern in a patient can provide diagnostic confidence, particularly for atypical-appearing individual lesions
Clinical Scenario
A 28-year-old man with red hair and Fitzpatrick skin type I presents with a 5 mm pink, firm papule on the left forearm that he has had for several years. Dermoscopy reveals a nonpigmented lesion with dotted vessels and shiny white streaks under polarized light. No pigment network is visible. The lesion dimples on lateral pressure. The patient has two other similar-appearing papules on the extremities.
What is your diagnosis and key dermoscopic findings?
Dermatofibroma (nonpigmented variant in fair skin)
In Fitzpatrick skin type I individuals (especially those with red hair), dermatofibromas may present as completely nonpigmented lesions showing only dotted vessels and shiny white streaks -- a pattern that can mimic Spitz nevus or amelanotic melanoma. The positive dimple sign on lateral compression and the presence of multiple lesions with consistent morphology across the patient's body strongly support dermatofibroma. The shiny white streaks correspond to dense collagen fibers in the papillary dermis (visible only with polarized dermoscopy due to birefringence). When melanoma cannot be excluded in isolated nonpigmented papules, biopsy is warranted.
4.14 Differential Diagnosis
Dermatofibromas must be differentiated from several important entities:
Melanoma
- Dermatofibromas with atypical pigment network, irregularly distributed pigment, or blue-red structureless areas may closely mimic melanoma
- The "white network" of dermatofibroma can be confused with the negative (inverse) network of melanoma
- Aneurysmal/hemosiderotic variants with blue-violet structureless pigmentation can be mistaken for melanoma
- Management: When melanoma cannot be confidently excluded, histopathologic evaluation is mandatory
Spitz Nevus
- Nonpigmented dermatofibromas with dotted vessels and shiny white streaks (especially in fair-skinned, red-haired individuals) enter the differential with Spitz nevus
- The dimple sign and presence of multiple similar lesions help distinguish dermatofibroma
Basal Cell Carcinoma (BCC)
- Dermatofibromas may display arborizing-like vessels, particularly the hemosiderotic variant
- The delicate pigment network of dermatofibroma is not a typical feature of BCC
- BCC-specific structures (leaf-like areas, spoke-wheel structures, blue-gray ovoid nests) are absent in dermatofibroma
Dermatofibrosarcoma Protuberans (DFSP)
- Both are fibrohistiocytic tumors, but DFSP is a malignant neoplasm requiring wide excision
- DFSP tends to be larger, present as a plaque, and lacks the dimple sign
- Dermoscopic overlap can occur; histopathology is the definitive discriminator
Amelanotic Melanoma
- Nonpigmented dermatofibromas with a central white patch, shiny white streaks, and polymorphous vessels may resemble amelanotic or hypomelanotic melanoma
- The overall pattern and dimple sign help differentiate
Key Takeaways
- Dermatofibromas with atypical pigment network, blue-red structureless areas, or arborizing-like vessels can closely mimic melanoma or BCC and require histopathologic confirmation.
- The dimple (Fitzpatrick) sign combined with consistent morphology across multiple lesions strengthens the clinical diagnosis of dermatofibroma.
- Ten classified dermoscopic patterns exist, grouped by presence or absence of peripheral pigment network, with the atypical pattern (6%) being the most diagnostically challenging.
5. Dermoscopic Features Reference Table
Table 5A: The Ten Dermoscopic Patterns of Dermatofibroma
| Pattern | Description | Prevalence (%) |
|---|---|---|
| 1 | Delicate pigment network throughout | 15 |
| 2 | Peripheral delicate pigment network and central white structureless patch | 35 |
| 3 | Peripheral delicate pigment network and central white structureless patch with ring-like globules | 9 |
| 4 | Peripheral delicate pigment network and central homogeneous pigmentation | 5 |
| 5 | Central white structureless patch with ring-like globules | 2 |
| 6 | Structureless pigmentation throughout | 5 |
| 7a | White structureless patch throughout | 6 |
| 7b | Multiple focal white structureless patches | 6 |
| 8 | Peripheral structureless pigmentation and central white structureless patch | 7 |
| 9 | Peripheral structureless pigmentation and central white structureless patch with ring-like globules | 5 |
| 10 | Atypical (cannot be classified into patterns 1--9) | 6 |
Source: Adapted from Zaballos, P., et al., Arch Dermatol, 144(1), 75--83, 2008. Percentages do not sum to 100% due to rounding.
Grouping:
- Patterns with peripheral delicate pigment network: 1, 2, 3, 4
- Patterns without peripheral delicate pigment network: 5, 6, 7a, 7b, 8, 9, 10
Table 5B: Individual Dermoscopic Features and Their Frequency
| Feature | Frequency (%) | Notes |
|---|---|---|
| Pigment network (any) | 72 | Typical delicate in most; atypical/broadened in 3% |
| Central structureless white patch | 57 | Most often single, well-demarcated, central |
| Structureless pigmentation | 25 | Peripheral (55%), throughout (24%), central (24%), irregular (3%) |
| Ring-like globules | Present in Patterns 3, 5, 9 | Round/oval, periphery darker than center |
| Shiny white structures (polarized only) | Common | Blotches and streaks within the white patch |
| Vascular structures (any) | Variable | Dotted, comma, hairpin, glomerular, linear; polymorphous; vascular blush |
| Scale | Less prevalent | -- |
| Ulceration/erosion | Less prevalent | More common in aneurysmal variant |
| Fissures and ridges | Less prevalent | Associated with SK-like variant |
| Mammillated surface | Less prevalent | Composed of ring-like globules |
Table 5C: Features by Dermatofibroma Variant
| Variant | Key Dermoscopic Features |
|---|---|
| Classic | Peripheral delicate network, central white structureless patch, ring-like globules, shiny white structures (polarized) |
| Aneurysmal / Hemosiderotic | Central bluish/reddish structureless area, shiny white streaks, peripheral network, polymorphous/branched vessels, yellowish peripheral areas, violaceous-blue structureless zones; in dark skin: white ring around central ulceration |
| Atrophic | Patchy delicate network, multiple white structureless areas |
| Seborrheic keratosis-like | Ridges and fissures, comedo-like openings, milia-like cysts, variable peripheral network and ring-like globules |
| Lipidized | Yellowish structureless pigmentation, yellow clods; may have central white patch with peripheral network |
| Sebaceous induction | Whitish or white-yellow lobules |
6. Differential Diagnosis Table
| Feature | Dermatofibroma | Melanoma | Spitz Nevus | BCC | DFSP |
|---|---|---|---|---|---|
| Clinical | Firm papule <1 cm, dimple sign positive | Asymmetric, irregular borders, variable color, growing | Dome-shaped, often pink or pigmented, young patients | Pearly papule/nodule, telangiectasia, possible ulceration | Firm plaque, usually >1 cm, slow-growing, dimple sign negative |
| Pigment network | Delicate, fine, lacey; fades peripherally | Atypical -- broadened, irregular lines and holes | Absent or reticular/globular | Absent (not a feature of BCC) | Variable |
| Central pattern | White structureless patch | Blue-whitish veil, regression, multicomponent | Starburst or globular pattern centrally | Blue-gray ovoid nests, leaf-like areas | Variable structureless areas |
| Ring-like globules | Present, round/oval, darker periphery | Irregular dots/globules | Peripheral globules (starburst) | Absent | Absent |
| Shiny white structures | Common (polarized), within white patch | Shiny white streaks (chrysalis) can occur | Can be present | Shiny white blotches and strands typical | Shiny white structures may occur |
| Vessels | Dotted, comma, hairpin, polymorphous (non-specific) | Polymorphous, atypical (linear irregular, milky-red areas) | Dotted vessels | Arborizing (thick, branching) vessels -- highly specific | Arborizing-like vessels reported |
| White network | Present (ring-like globules + collagen) | Negative (inverse) network | Negative network possible | Absent | Not typical |
| Dimple sign | Positive (pathognomonic) | Negative | Negative | Negative | Negative |
| Action | Monitor or excise if atypical | Excise | Excise or monitor depending on features and age | Biopsy and treat | Wide excision required |
7. Clinical Pearls
The classic triad: A central white structureless patch + delicate peripheral pigment network + positive dimple sign is virtually diagnostic of dermatofibroma. This combination is present in roughly one-third of all cases.
Always check polarized AND nonpolarized: Shiny white structures are only visible with polarized dermoscopy, while superficial epidermal features (fissures, comedo-like openings) are better seen with nonpolarized dermoscopy. Contact versus noncontact technique further alters vascular findings.
Ring-like globules are a clue: These round/oval structures with a darker periphery, found near the center of the lesion, are characteristic of dermatofibroma and represent flattened, widely spaced hyperpigmented rete ridges. Their presence, even without a typical peripheral network, should raise the diagnosis.
White network versus negative network: The "white network" of dermatofibroma (collagen surrounding islands of pigmented rete ridges) can mimic the negative (inverse) network seen in melanoma. When in doubt, the dimple sign and clinical context (firm papule, extremity, <1 cm) favor dermatofibroma.
Aneurysmal variants demand caution: Hemosiderotic and aneurysmal dermatofibromas with blue-red structureless areas, polymorphous vessels, and atypical patterns are a recognized melanoma mimic. When these features are present, histopathologic evaluation should be strongly considered.
Body site matters: The trunk favors structureless pigmentation patterns, while the extremities favor the classic central white patch with peripheral network. The face and hands favor network throughout the lesion. Interpret findings in the context of anatomic location.
Skin phototype matters: In darker skin types (IV--VI), the classic pattern is less prevalent. Expect a grayer central patch and more darkly pigmented ring-like globules. In very fair skin (type I), dermatofibromas may be entirely nonpigmented, mimicking Spitz nevus or amelanotic melanoma.
The 3% atypical rule: Approximately 3% of dermatofibromas show an atypical or broadened pigment network. These lesions should be excised for histopathologic confirmation, as they cannot be confidently distinguished from melanoma on dermoscopy alone.
SK-like features do not exclude dermatofibroma: Ridges, fissures, comedo-like openings, and milia-like cysts can occur when dermatofibromas have superimposed epidermal changes. Look for underlying typical features (peripheral network, ring-like globules) beneath the keratotic surface.
Yellow means lipidized: Yellowish structureless pigmentation or yellow clods should prompt consideration of lipidized dermatofibroma, a specific histologic variant with foamy cytoplasm cells.
Clinical Scenario
A 28-year-old woman presents with a firm, 7 mm brown papule on her anterior shin that has been stable for over two years. Dermoscopy reveals a central white structureless patch surrounded by a delicate, fine pigment network that fades gradually into the surrounding skin. Under polarized light, shiny white streaks are visible within the central patch. Lateral compression produces a dimple.
What is your diagnosis?
Dermatofibroma (classic pattern)
This lesion displays the classic triad of dermatofibroma: a central white structureless patch (correlating with attenuated epidermis over fibrous stroma), a delicate peripheral pigment network (correlating with hyperpigmented basal keratinocytes along elongated rete ridges), and a positive dimple sign. The shiny white structures visible under polarized light correspond to dense collagen fibers in the papillary dermis. This Pattern 2 presentation is the most common dermoscopic pattern, seen in approximately 35% of dermatofibromas.
Clinical Scenario
A 45-year-old man presents with a 6 mm reddish-blue nodule on his right thigh that appeared several months ago after minor trauma. Dermoscopy shows a central bluish structureless area with shiny white streaks, a peripheral delicate pigment network, and prominent branched (arborizing-like) vessels. A yellowish structureless area is noted at the periphery.
What is your diagnosis?
Aneurysmal (hemosiderotic) dermatofibroma
The central bluish structureless area with shiny white streaks, peripheral delicate network, and prominent branched vessels are characteristic of the aneurysmal/hemosiderotic variant. The yellowish peripheral area correlates with hemosiderin or foamy histiocytes. Although the arborizing-like vessels could raise concern for BCC, the presence of a delicate peripheral pigment network (not a feature of BCC) supports dermatofibroma. However, these dermoscopic features are not entirely specific, and melanoma cannot be confidently excluded. Histopathologic evaluation is recommended.
Clinical Scenario
A 32-year-old woman with Fitzpatrick skin type I and red hair presents with a 5 mm pinkish papule on her left forearm. Dermoscopy reveals only dotted vessels and shiny white streaks without any pigment network. The lesion is firm, and she has two other similar papules on her legs that have been present for years. Lateral compression produces a dimple.
What is your diagnosis?
Nonpigmented dermatofibroma (in fair skin)
In very fair-skinned, red-haired individuals (Fitzpatrick skin type I), dermatofibromas may present as entirely nonpigmented lesions showing only dotted vessels and shiny white streaks. This appearance closely mimics Spitz nevus and amelanotic melanoma. The positive dimple sign and the presence of multiple similar lesions on the extremities are critical diagnostic clues that support dermatofibroma over its malignant mimics. Without these clinical features, biopsy would be warranted.
9. Textbook Cross-References
| Topic | Textbook Page(s) | Figures / Tables |
|---|---|---|
| Chapter 6a: Dermatofibroma (full section) | pp. 90--96 | Figures 6a.1--6a.26, Table 6a.1 |
| Classic pattern (central white patch + peripheral network) | p. 90 | Figures 6a.2--6a.7 |
| Ring-like globules | p. 90 | Figures 6a.6, 6a.8, 6a.16 |
| Pigment network statistics (Zaballos et al.) | pp. 90--91 | -- |
| White structureless patch statistics | pp. 91, 93 | -- |
| Vascular patterns | p. 91 | Figures 6a.4, 6a.15, 6a.19 |
| Ten dermoscopic patterns | pp. 91--92 | Table 6a.1, Figure 6a.1 |
| Anatomic location influence | p. 91 | -- |
| Skin type influence | p. 91 | Figures 6a.20, 6a.24 |
| Aneurysmal/hemosiderotic variant | pp. 91--93 | Figures 6a.8--6a.9, 6a.13, 6a.21, 6a.25 |
| Atrophic variant | p. 93 | -- |
| SK-like features | pp. 93--95 | Figures 6a.16--6a.17 |
| Lipidized variant | p. 95 | Figures 6a.12, 6a.23 |
| Sebaceous induction | p. 95 | -- |
| Nonpigmented dermatofibroma (fair skin) | p. 94 | Figures 6a.22, 6a.26 |
| Polarized vs. nonpolarized technique | p. 90 | Figures 6a.2--6a.3, 6a.19 |
| Conclusion and management | p. 95 | -- |
| References | p. 96 | References 1--17 |
10. Related Modules
| Module | Relevance |
|---|---|
| Module 01: Introduction and Principles of Dermoscopy | Understanding polarized versus nonpolarized dermoscopy and contact versus noncontact technique, which critically affect dermatofibroma appearance |
| Module 02: Histopathologic Correlations | Histopathologic basis for pigment network (rete ridges), structureless white areas (fibrosis), shiny white structures (collagen), and the dermatofibroma correlates discussed in Chapter 3 |
| Module 04: Top-Down 2-Step Algorithm -- Level 2 | Application of Level 2 analysis to determine whether a lesion is melanocytic or nonmelanocytic; dermatofibroma classification within the nonmelanocytic pathway |
| Module 05: Prediction without Pigment | Algorithm for nonpigmented lesions, directly applicable to nonpigmented dermatofibromas in fair-skinned individuals |
| Module 06: Chaos and Clues | Triage algorithm to assess whether a dermatofibroma with atypical features warrants excision |
| Module 09: Basal Cell Carcinoma | Differential diagnosis -- distinguishing arborizing vessels and blue-gray structures of BCC from dermatofibroma features |
| Module 12: Solar Lentigines, Seborrheic Keratoses, LPLK | Differential for dermatofibromas with SK-like epidermal changes |
| Module 19: Spitz and Reed Nevi | Differential diagnosis for nonpigmented dermatofibromas that mimic Spitz nevus |
| Module 21: Superficial Spreading Melanoma | Understanding atypical network and negative network features that may overlap with dermatofibroma white network |
| Module 26: Amelanotic and Hypomelanotic Melanoma | Differential for nonpigmented dermatofibromas with polymorphous vessels and shiny white structures |
Module 08 corresponds to Atlas of Dermoscopy, 3rd Edition, Chapter 6a (pp. 90--96). This module is part of Part III: Nonmelanocytic Lesions in the Dermoscopy Educational Course.
Image Sources & Citations
- DERM12345 (Skin Lesion Dataset with 40 Subclasses): DERM12345: A Large-scale Skin Lesion Image Dataset with 40 Subclasses. Figshare. 2023. License: CC-BY-4.0.