Module 05: Prediction without Pigment
A Decision Algorithm for Nonpigmented Skin Lesions
Source: Dermoscopy Educational Course
1. Learning Objectives
After completing this module, you should be able to:
- Define what constitutes a "nonpigmented" lesion for the purposes of the Prediction without Pigment algorithm (absence of melanin-based pigmentation; brown and gray color absent).
- List the red flags that warrant formal algorithmic assessment of a nonpigmented lesion, including patient concern, clinical pattern-breaker, ulceration, surface keratin on raised lesions, and polarizing-specific white lines.
- Apply the three-step Prediction without Pigment algorithm in sequential order: ulceration assessment, white clue evaluation, and vessel pattern analysis.
- Identify white clues (white lines, surface keratin, white structureless areas, and white circles) and explain their diagnostic significance, particularly the specificity of white circles for SCC/KA.
- Classify vessel structures into the eight standard types (dots, clods, linear straight, linear looped, linear curved, linear serpentine, linear helical, linear coiled) and describe the morphology of each.
- Classify vessel arrangements into the eight standard categories (random, clustered, serpiginous, linear, centered, radial, reticular, branched) and describe each pattern.
- Recognize the four benign monomorphous vessel patterns (clods-only, centered, serpiginous, reticular) and their associated diagnoses, including the caveats that limit their application.
- Distinguish polymorphous vessel patterns that raise suspicion for malignancy, particularly the combination of dotted vessels with linear vessels as a clue to melanoma.
2. Prerequisites
- Module 01: Introduction and Principles of Dermoscopy -- understanding of polarized vs. nonpolarized dermoscopy is essential for recognizing white lines.
- Module 02: Histopathologic Correlations -- understanding of how dermatoscopic structures correlate with histopathology (vessels, keratin, white structures).
- Module 03: Pattern Analysis Revised -- familiarity with basic structural elements (lines, dots, clods, circles, structureless areas) and the concept of pattern recognition.
3. Key Concepts
The Challenge of Nonpigmented Lesions
Pigmented structures (network, globules, streaks, blotches) provide the foundation for most dermoscopic algorithms. When melanin-based pigmentation is absent, the clinician loses these familiar landmarks and must rely on a different set of clues: ulceration, white structures, and vascular patterns. This makes the dermatoscopic evaluation of nonpigmented lesions inherently more challenging.
Definition of a Nonpigmented Lesion
For the purposes of this algorithm, a nonpigmented lesion is one without clinical or dermatoscopic evidence of pigmentation due to melanin:
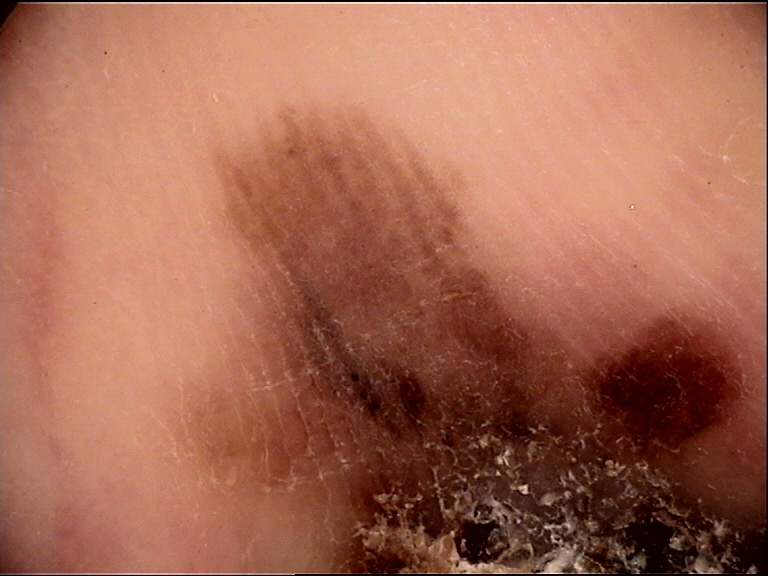
- Brown or gray color must be absent. If either is present, the lesion should be assessed as a pigmented lesion using Chaos and Clues or another pigmented-lesion algorithm.
- Black, purple, or blue colors may be present only if they are attributable to blood rather than melanin. This is usually the case when these colors are associated with red color only (i.e., vascular origin).
- If pigmented structures are present even focally, the lesion is generally best assessed as a pigmented lesion.
Relationship to Other Algorithms
Prediction without Pigment is the nonpigmented counterpart of Chaos and Clues (Module 06), which is used for pigmented lesions. Both are algorithmic methods that use pattern analysis to guide the clinician to a biopsy decision (biopsy indicated vs. not indicated), rather than directly arriving at a specific histopathologic diagnosis. However, revised pattern analysis can be applied after the algorithmic assessment to predict a specific diagnosis.
4. Core Content
4.1 Rationale for a Dedicated Nonpigmented Algorithm
The most common nonpigmented malignancies encountered in dermoscopy practice include basal cell carcinoma (BCC), squamous cell carcinoma (SCC), keratoacanthoma (KA), and amelanotic/hypomelanotic melanoma. These lesions lack the melanin-based structures that power algorithms designed for pigmented lesions. Therefore, a dedicated approach is needed that exploits the clues that are available in nonpigmented lesions:
- Ulceration -- extremely common in BCC and visible clinically or via adherent fiber dermatoscopically.
- White structures -- white lines (polarizing-specific or nonpolarized), surface keratin, white structureless areas, and white circles.
- Vessel patterns -- the morphology and arrangement of blood vessels, which are often the dominant dermatoscopic feature when pigment is absent.
The algorithm is designed for use when the lesion cannot be confidently classified as one of the six common benign nonpigmented entities by pattern recognition alone: nonpigmented nevus, benign keratinocytic lesion (including viral warts and actinic keratoses), hemangioma, dermatofibroma, sebaceous gland hyperplasia, or cyst.
4.2 Red Flags for Nonpigmented Lesions
Just as pigmented lesions are selected for dermatoscopic analysis by recognizing "red flags," the same principle applies to nonpigmented lesions. Red flags are features that classify a lesion as suspicious and warrant formal algorithmic assessment.
Red Flag 1: Patient Concern or Clinical Evidence of Change
- Lesions of concern to the patient should never be dismissed without close examination including dermoscopy.
- Patient concern should automatically flag a lesion as suspicious.
- Documented evidence of change at mature age flags a lesion as suspicious.
- Any elevated, firm, and continuously growing (EFG) lesion should be subjected to excision biopsy.
Red Flag 2: Clinical Pattern-Breaker
- The disorganized and uncontrolled behavior of malignant neoplasms causes nonpigmented malignant lesions to break the pattern of the surrounding skin lesions.
- Malignant neoplasms may have an irregular, unexpected shape or larger size compared with surrounding lesions due to their unrestrained growth.
- Any lesion that clinically breaks the pattern should be flagged as suspicious and analyzed with dermoscopy.
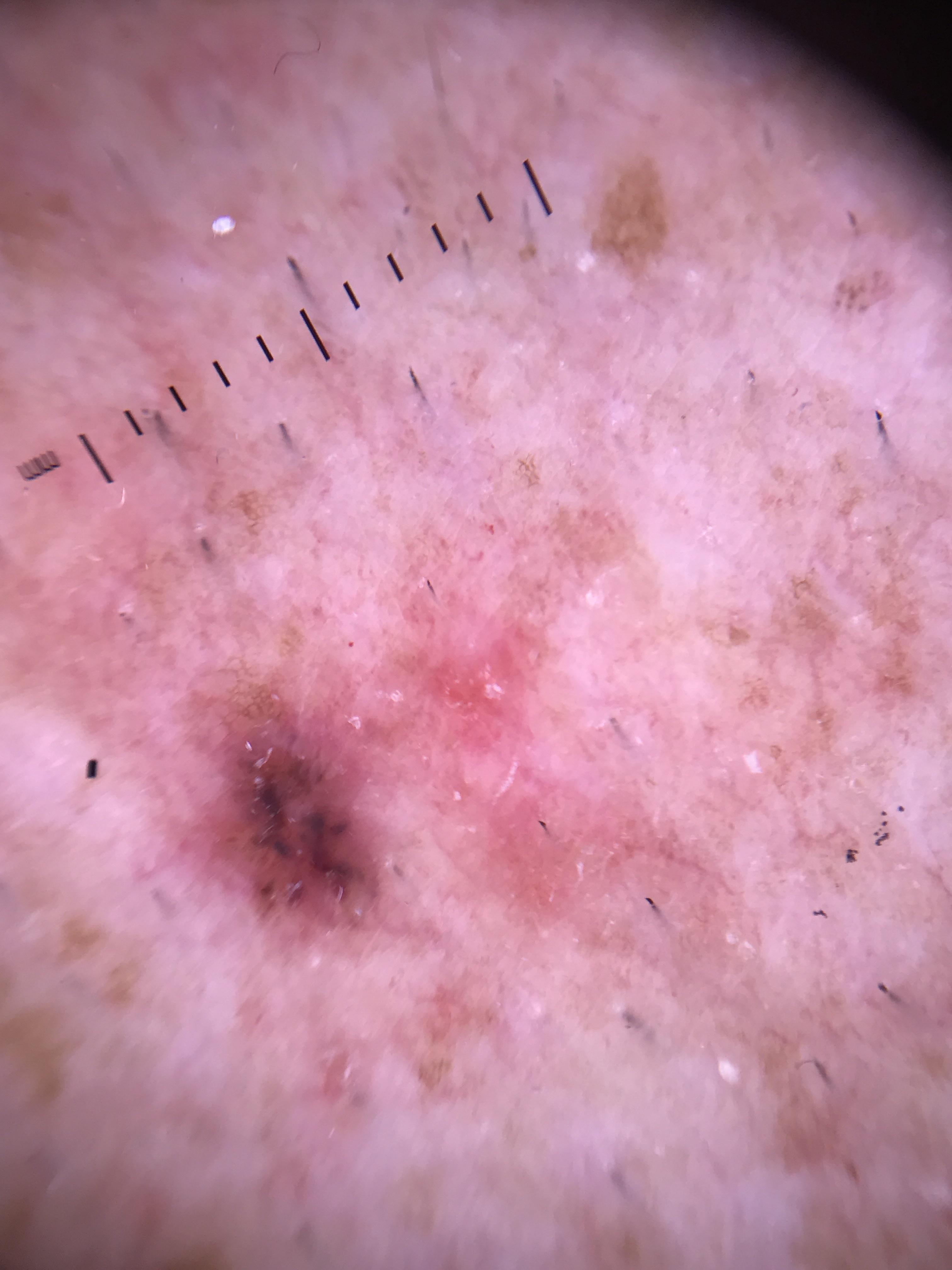
Red Flag 3: Ulceration
- Ulceration visible clinically or dermatoscopically on a lesion of concern (see Step 1 of the algorithm).
Red Flag 4: Surface Keratin on a Raised Lesion
- Surface keratin on a raised nonpigmented lesion is a clinical red flag warranting further assessment.
Red Flag 5: Polarizing-Specific White Lines
- White lines recognized during dermatoscopic evaluation, particularly with polarized light, are a red flag warranting formal assessment.
Check Your Understanding
What are the key vascular patterns to look for in nonpigmented (amelanotic) lesions?
Key vascular patterns include dotted vessels (melanocytic lesions), arborizing vessels (BCC), hairpin/looped vessels (keratinizing tumors like SCC and seborrheic keratosis), glomerular vessels (Bowen disease), and polymorphous vessels (melanoma). The pattern and distribution of vessels are the primary diagnostic clues.
Key Takeaways
- Nonpigmented lesions require a dedicated algorithm because standard pigment-based rules cannot be applied when melanin is absent.
- Ulceration in a nonpigmented lesion that is not explained by trauma is a strong indicator of malignancy (BCC, SCC, or amelanotic melanoma).
- White structures (shiny white lines, white circles) visible under polarized dermoscopy provide critical diagnostic information in nonpigmented lesions.
4.3 The Prediction without Pigment Algorithm: Step-by-Step
The algorithm proceeds in a strict hierarchical order. Each step takes priority over subsequent steps. The rationale for this ordering is:
- Ulceration is given first priority because BCC is the most common nonpigmented skin malignancy and ulceration is frequently present.
- White clues are given second priority because keratin clues (surface keratin, white structureless areas, white circles) have been shown to be more robust than vessel clues for raised nonpigmented lesions.
- Vessel pattern analysis is the final step, employed only when ulceration and white clues are absent.
Step 1: Is There Ulceration?
Rationale: BCC is the most common nonpigmented skin malignancy, and ulceration is frequently present on its surface. If ulceration is observed on a lesion of concern, this alone is sufficient to warrant biopsy consideration.
Clinical Assessment of Ulceration:
- Ulceration is often best assessed clinically (naked-eye examination).
- If ulceration of a lesion of concern is observed with the naked eye, this increases the appropriateness of dermatoscopic examination -- additional dermatoscopic clues can add weight to the suspicion of malignancy and provide evidence for a precise diagnosis.
Dermatoscopic Assessment of Ulceration:
- Dermoscopy may actually make ulceration more difficult to appreciate because immersion fluid or polarized light may render the optical features of ulceration invisible.
- Adherent fiber is a key dermatoscopic clue to ulceration: ulceration results in a serum exudate that may trap clothing fiber or other environmental/intrinsic matter (including hair). This clue can reveal even micro-ulceration that is not apparent clinically.
Secondary Effects of Ulceration:
- Ulceration promotes neoangiogenesis, which can produce different vessel morphologies including a polymorphous vessel pattern.
- Ulceration can promote secondary keratinization, resulting in surface keratin or white circles -- structures normally expected in SCC but not in BCC.
Differential Diagnosis of Ulcerated Nonpigmented Lesions:
- Basal cell carcinoma (most common)
- Squamous cell carcinoma
- Amelanotic melanoma
- Traumatic ulceration (should not be a confounding factor if the dermatoscope is applied to lesions of genuine concern)
Decision: If ulceration is present --> consider biopsy. Proceed with further dermatoscopic analysis to predict the specific diagnosis.
Step 2: White Clues
Definition: "White clues" encompass two categories:
Category A -- White Lines (applicable to any nonpigmented lesion, flat or raised):
- White lines must be at least as white as the perilesional skin.
- May be seen with nonpolarized and/or polarized dermoscopy.
- Polarizing-specific white lines are the white lines most frequently seen in nonpigmented lesions: straight lines, orientated perpendicularly to each other, not crossing, and frequently shifting as the dermatoscope is rotated.
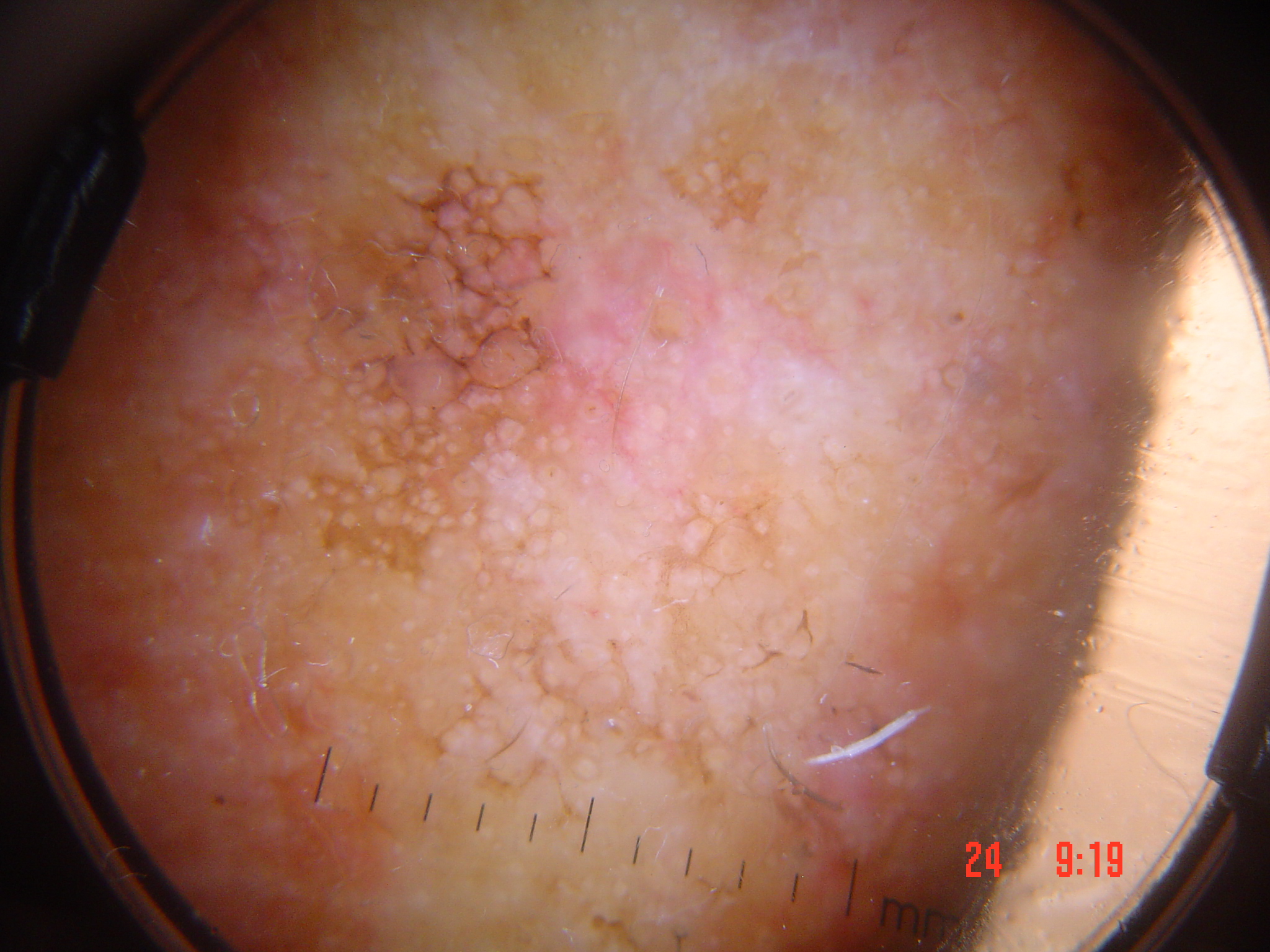
Category B -- Keratin Clues (applicable only to raised nonpigmented lesions):
- Surface keratin -- visible clinically or dermatoscopically. Because dermoscopy is designed to render keratin invisible, surface keratin is often best displayed clinically but generally also seen dermatoscopically in raised lesions.
- White structureless areas -- a dermatoscopic clue corresponding to significant acanthosis of highly keratinized squamous cells. If present, the lesion will be raised (not flat), because a flat keratinizing lesion would not have this clue.
- White circles -- a dermatoscopic clue. The most useful of the three keratin clues: 87% specific for SCC/KA in a consecutive test series, with 44% of SCC/KA displaying dermatoscopic white circles. White circles have frequently enabled the confident prediction of very small SCC where such a diagnosis would not have been possible prior to this clue being described.
Definition of "Raised": A raised lesion is one that is visibly or palpably raised (other than due to surface keratin alone), or a lesion that has the dermatoscopic clue to a raised lesion -- looped vessels.
Diagnostic Associations of White Clues:
| White Clue | Primary Association | Other Associations |
|---|---|---|
| Polarizing-specific white lines | BCC (most frequent) | SCC in situ, LPLK, amelanotic melanoma, dermatofibroma, Spitz nevus |
| Surface keratin (raised lesion) | SCC / KA | Ulcerated BCC (secondary keratinization) |
| White structureless areas (raised) | SCC / KA | Ulcerated BCC (secondary keratinization) |
| White circles (raised lesion) | SCC / KA (87% specific) | Actinic keratosis (but AK is not raised) |
Important Caveats:
- Actinic keratoses may have surface keratin and/or white circles, but these lesions are not raised and are therefore not predicted to harbor invasive malignancy; they may be suitable for nonsurgical treatment without biopsy.
- The keratin clue of white structureless areas is not expected in a flat keratinizing lesion.
- When white lines are present, they take priority over vessel analysis. White lines should lead to excision even if there is a monomorphous pattern of centered vessels (which would otherwise suggest benignity).
- Vessel clues serve as additional evidence to help predict a specific diagnosis when white lines are present (e.g., polymorphous vessels including dotted vessels favor melanoma over BCC).
Decision: If any white clue is present --> consider biopsy. Use vessel patterns as supplementary evidence for predicting the specific diagnosis.
Clinical Scenario
A 74-year-old man presents with a firm, raised, flesh-colored nodule on the right temple that appeared 4 months ago and has been slowly enlarging. Clinically, there is a central crust suggestive of ulceration. Dermoscopy reveals an adherent fiber trapped in a serum exudate, confirming micro-ulceration. Additionally, bright red serpentine vessels with distinct branching (arborizing pattern) are visible on a translucent background.
What is your diagnosis and key dermoscopic findings?
Basal cell carcinoma (nodular type)
Applying the Prediction without Pigment algorithm: Step 1 asks about ulceration -- the adherent fiber is a key dermatoscopic clue confirming micro-ulceration, even when the ulceration itself may be difficult to appreciate under dermoscopy. This alone warrants biopsy consideration. The arborizing (branched serpentine) vessels on a translucent stroma are the characteristic vessel pattern of BCC, providing supplementary diagnostic evidence. BCC is the most common nonpigmented skin malignancy, and ulceration is its most frequently encountered clinical and dermatoscopic feature.
Step 3: Is the Vessel Pattern Consistent with Malignancy?
It is only when the nonpigmented lesion of concern has neither ulceration nor white clues that analysis of vessel patterns becomes the primary assessment tool. If either of the higher-priority clues is present, vessels should be considered as additional clues to a specific diagnosis rather than being relied on to avoid a biopsy.
4.3.1 Vessel Morphology Classification
Revised pattern analysis defines eight types of vessel structures and eight types of vessel arrangements.
Eight Vessel Structure Types:
| Vessel Type | Morphologic Description |
|---|---|
| Dot | A vessel structure, red in color, too small to have a discernible shape (at 10x magnification) |
| Clod | A well-circumscribed solid vessel structure, red or purple in color, larger than a dot, any shape |
| Linear straight | Linear vessels without a bend |
| Linear looped | Linear vessels with one sharp bend (180 degrees) resulting in a reversal of direction (U-turn) |
| Linear curved | Linear vessels with one gentle bend |
| Linear serpentine | Linear vessels with more than one bend and shaped in a snakelike fashion |
| Linear helical | Linear vessels with multiple bends twisted along a central axis |
| Linear coiled | Linear vessels with multiple bends and convoluted compactly |
Relationship Between Vessel Morphology and Dermal Papilla Architecture:
- A vessel within the dermal papilla ascending to the top and curving across before descending appears as a curved vessel.
- If the vessel is convoluted, it appears as a coiled vessel.
- If the vessel turns on itself sharply, it appears as a dot.
- Once a lesion becomes raised, the dermal papilla distorts laterally, and whatever the dermatoscopic appearance was projects as a looped vessel.
Eight Vessel Arrangement Types:
| Arrangement | Definition |
|---|---|
| Random | Vessels not arranged in any of the specific ways listed below |
| Clustered | Vessels that are concentrated in certain areas of a lesion |
| Serpiginous | Dotted or coiled vessels arranged in a linear snakelike pattern (distinct from the "linear serpentine" vessel type) |
| Linear | Dotted or coiled vessels arranged in straight lines |
| Centered | Vessels located at the center in skin-colored clods |
| Radial | Linear vessels in a group orientated from the periphery towards the center of a lesion but not crossing it |
| Reticular | Linear vessels crossing at right angles to form a net-like pattern |
| Branched | Linear serpentine vessels that divide into consecutively thinner serpentine vessels from a central main stem |
4.3.2 Monomorphous vs. Polymorphous Patterns
- Monomorphous pattern: One vessel type predominates.
- Polymorphous pattern: More than one vessel type is present in significant numbers within a pattern, or there are separate patterns of more than one vessel type.
- A few scattered vessels of a second type among a dominant pattern do not constitute a polymorphous pattern. For example, a pattern of linear serpentine vessels with a couple of dot vessels is not polymorphous. There would need to be enough dotted vessels either to clearly interfere with the serpentine vessel pattern or to form a separate cluster making a pattern of their own.
4.3.3 The Four Benign Monomorphous Vessel Patterns
When seen in a nonpigmented skin lesion without ulceration or white clues, the following four monomorphous patterns are consistent with a benign diagnosis:
1. Clods-Only Pattern --> Hemangioma
- A pattern of red, purple, and/or blue clods-only is consistent with hemangioma in an apparently stable lesion.
- Hemangiomas are normally diagnosed with confidence clinically; the dermatoscopist should examine thousands to become familiar with their distinctive but protean morphology.
- Caveat: While the rule states that clods-only excludes linear vessels, it is not uncommon to see hemangiomas with some linear vessels in addition to clods, particularly in very small embryonic hemangiomas. Clinical correlation is required. If there is additional cause for concern (e.g., reported recent change), biopsy may be indicated, and the presence of any linear vessels increases the index of suspicion.
- Critical rule: Any apparent hemangioma with vessels seen within the red or purple clods should be excised.
2. Centered Vessel Pattern --> Verruca, Congenital Nevus, or Seborrheic Keratosis
- Vessels (any type) centered in skin-colored clods in an apparently stable lesion.
- Critical distinction: The clods must be skin-colored, not dark pink or red. A dark pink or red background can be seen in some nodular melanomas with vessels centered in pink clods.
- Priority rule: Any white lines take priority over vessel analysis -- white lines should lead to excision even if there is a monomorphous centered pattern, because some nodular melanomas also show white lines.
- Pressure artifact caveat: A background pink color can be falsely rendered as skin-colored if undue pressure is exerted on the dermatoscope foot-plate. Clinical observation of pink color should override dermatoscopic observation of skin color, and the centered pattern diagnosis should not be made.
3. Serpiginous Vessel Pattern --> Clear Cell Acanthoma
- A pattern of serpiginous vessels only (dotted or coiled vessels arranged in a linear snakelike pattern) is consistent with clear cell acanthoma.
- This pattern has no differential diagnosis -- it is pathognomonic.
4. Reticular Vessel Pattern --> Benign (Sun-Damaged Skin or Telangiectasia Macularis Perstans)
- A pattern of reticular vessels only (linear vessels crossing at right angles forming a net-like pattern) predictably corresponds to a benign diagnosis.
- Commonly seen in isolated patches on sun-damaged skin (representing the superficial horizontal vascular plexus made visible by solar-induced atrophy of the overlying dermis).
- Also seen in telangiectasia macularis perstans (a form of mastocytosis).
4.3.4 All Other Vessel Patterns: Assess for Biopsy
All vessel patterns other than the four benign monomorphous patterns should be assessed for biopsy in lesions of concern.
Polymorphous Vessel Patterns and Malignancy:
- Any polymorphous pattern of vessels can be a clue to malignancy.
- Important caveat: Benign lesions such as seborrheic keratoses and most dermal nevi can also have polymorphous (linear) vessels. The dermatoscopist is encouraged to examine thousands of obviously benign examples to become familiar with their protean vessel morphology.
Dotted Vessels + Linear Vessels = Suspicion for Melanoma:
- Any polymorphous vessel pattern that includes a pattern of dots in addition to any pattern of linear vessels raises suspicion for melanoma.
- This assumes the lesion is not an unequivocal seborrheic keratosis or dermal nevus (scattered linear and dot vessels are not uncommon in such benign lesions).
- A few dotted vessels in a lesion with predominantly linear vessels does not constitute a pattern of dotted vessels. The pattern of dotted vessels in melanoma will usually (but not always) appear as a separate pattern rather than speckled between linear vessels.
Why Dots Suggest Melanoma:
- Dotted vessels represent prominent dermal papillae vessels projecting vertically from the superficial vascular plexus towards the epidermis.
- Dots are only expected in the macular (flat) part of a melanoma.
- Once melanoma becomes invasive, the normal organized morphology of the dermal papillae becomes distorted with lateral displacement, meaning dermal papillae vessels project as linear vessels of various types.
- Linear vessels in melanoma may represent: laterally displaced dermal papillae vessels, dilated dermal plexus vessels (usually serpentine), or polymorphic linear vessels (looped, curved, serpentine, helical, or coiled).
Melanoma Vessel Patterns:
- A melanoma may have a polymorphous pattern of linear vessels without a pattern of dots, in which case the different vessel types are likely combined in a random arrangement.
- Linear vessels can be seen in both macular and raised portions of a melanoma.
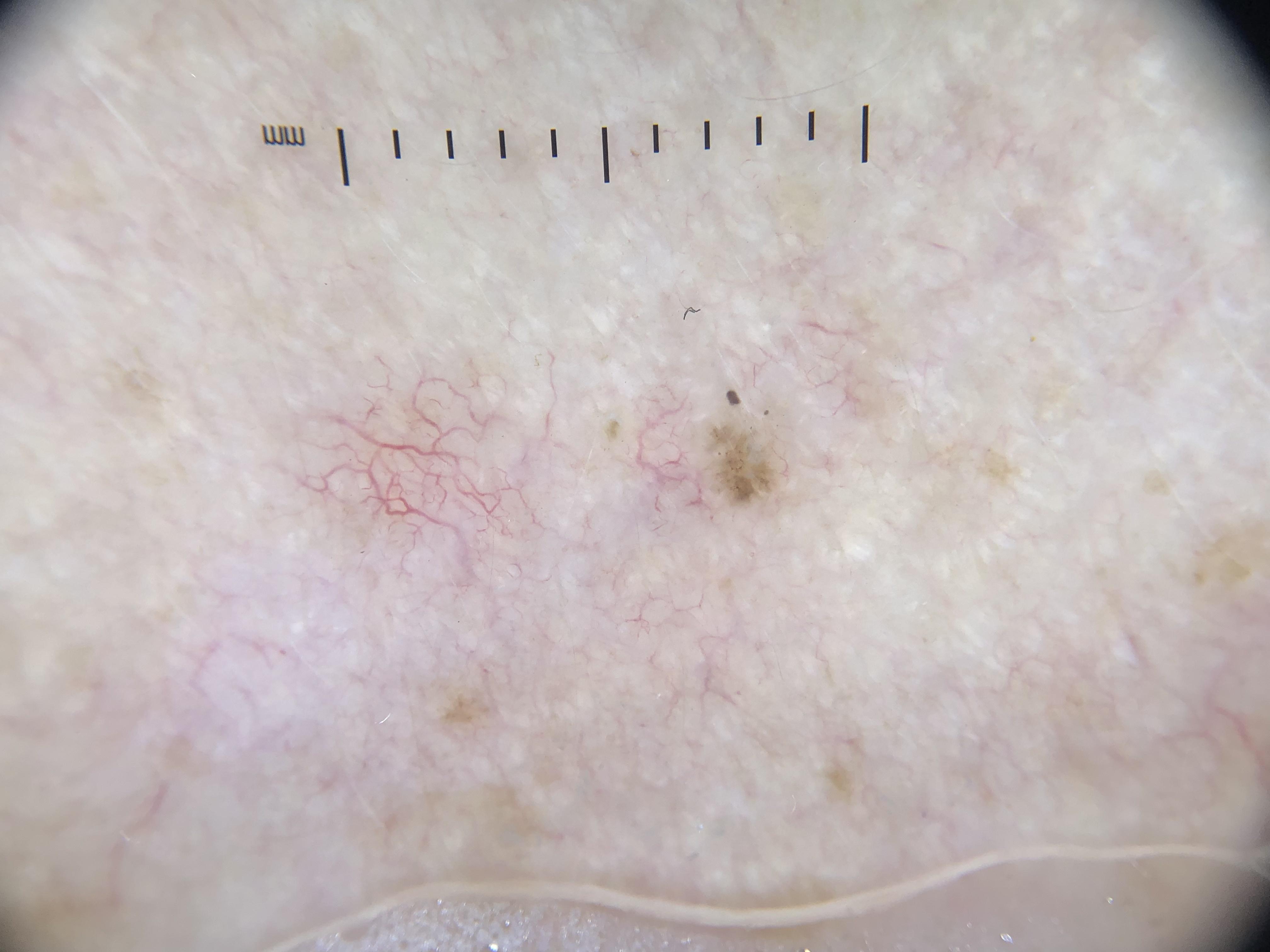
BCC Vessel Patterns:
- BCC characteristically shows a monomorphous pattern of branched serpentine (arborizing) vessels.
- These vessels are thrown into sharp relief by the translucent stroma characteristic of BCC.
- The serpentine-branched vessels may blend seamlessly with the perilesional superficial dermal vascular plexus; what is unique to BCC is the translucent stroma that casts the vessels into sharp relief.
Distinguishing BCC from Melanoma by Vessels:
- Vessel clues can often (but not always) distinguish BCC from melanoma when white lines are present in both.
- A polymorphous pattern including dotted vessels is a frequent feature of melanoma but not of BCC.
Clinical Scenario
A 63-year-old woman presents with a pink, slightly raised nodule on the left shin that has been growing for 3 months. There is no ulceration and no surface keratin. Dermoscopy with polarized light shows no white lines. Vessel analysis reveals two distinct vessel patterns: a cluster of dotted vessels in the flat peripheral area and serpentine linear vessels in the raised central portion. The arrangement is random and clearly polymorphous.
What is your diagnosis and key dermoscopic findings?
Amelanotic melanoma (suspected)
Applying the Prediction without Pigment algorithm: Step 1 (ulceration) is negative. Step 2 (white clues) is negative -- no white lines, no surface keratin, no white structureless areas, no white circles. Step 3 (vessel pattern analysis) becomes the primary assessment. The pattern is polymorphous (two vessel types in significant numbers), which falls outside the four benign monomorphous patterns and warrants biopsy assessment. Critically, the combination of dotted vessels plus linear vessels raises specific suspicion for melanoma. The dots represent prominent dermal papillae vessels in the flat macular portion, while the linear serpentine vessels reflect distorted dermal papillae architecture in the invasive raised portion.
Check Your Understanding
What vascular pattern is most characteristic of Bowen disease (squamous cell carcinoma in situ)?
Glomerular vessels (also called coiled vessels) are most characteristic of Bowen disease. They appear as tightly coiled vessels resembling the glomerular capillary tuft of the kidney and are typically arranged in clusters distributed across the lesion surface.
Key Takeaways
- The algorithm evaluates vessel morphology and pattern as the primary diagnostic criterion when pigment is absent.
- Arborizing vessels suggest BCC, glomerular vessels suggest SCC/Bowen disease, and polymorphous vessels with milky-red areas suggest amelanotic melanoma.
- A nonpigmented lesion with any dermoscopic structure (vessels, ulceration, white clues) that cannot be confidently diagnosed as benign warrants biopsy.
4.4 Application in Routine Practice
The practical workflow integrates pattern recognition with the formal algorithm:
- First: Attempt to identify the lesion as one of the six common benign nonpigmented entities by pattern recognition (nonpigmented nevus, benign keratinocytic lesion, hemangioma, dermatofibroma, sebaceous gland hyperplasia, cyst). These are ubiquitous, and expertise in their recognition can be achieved rapidly through deliberate practice.
- Second: Also attempt to identify malignant lesions (e.g., BCC) by pattern recognition, which becomes more frequent with increasing experience.
- Third: If pattern recognition is not possible, or if red flags are present, apply the Prediction without Pigment algorithm.
- Fourth: Use all available information -- both clinical and dermatoscopic -- when assessing nonpigmented lesions.
Important principle: The algorithm should not be regarded as an ultimate method set in stone. It is designed as a useful tool suitable for seamless integration into routine practice. Clinicians are encouraged to use it as a framework on which to organize their accumulated experience and to adapt and individualize the method.
Check Your Understanding
Why is the 'Prediction without Pigment' approach important in clinical dermoscopy?
Many clinically important lesions, including amelanotic melanoma and nonpigmented BCC, lack the pigmented structures that traditional dermoscopic algorithms rely on. Without the ability to evaluate nonpigmented features (especially vascular patterns and white structures), these potentially dangerous lesions may be missed or misdiagnosed.
Key Takeaways
- Combining the nonpigmented algorithm with polarized dermoscopy maximizes detection of amelanotic melanoma, which is the most commonly missed skin cancer.
- Dotted vessels alone are nonspecific and can appear in many lesions; their diagnostic value increases when combined with other vessel types (polymorphous pattern).
- Serial monitoring is generally not appropriate for suspicious nonpigmented lesions because amelanotic melanoma can progress rapidly.
5. Vessel Pattern Reference Table
Vessel Structure Types
| Vessel Structure | Morphology | Typical Associations |
|---|---|---|
| Dot | Red, too small to have discernible shape at 10x | Melanoma (macular component); dermal papillae vessels projecting vertically |
| Clod | Well-circumscribed, solid, red/purple, larger than dot | Hemangioma (clods-only pattern); vascular lesions |
| Linear straight | Linear vessel without any bend | Component of polymorphous patterns |
| Linear looped | One sharp 180-degree bend (U-turn) | Raised lesions (dermal papillae displaced laterally); SCC (raised component) |
| Linear curved | One gentle bend | Dermal papillae vessels curving across papilla; component of polymorphous patterns |
| Linear serpentine | Multiple bends, snakelike shape | BCC (branched arrangement = arborizing vessels); dilated dermal plexus vessels |
| Linear helical | Multiple bends twisted along central axis | Component of polymorphous patterns in malignancy |
| Linear coiled | Multiple bends, convoluted compactly | SCC in situ (coiled vessels at periphery); clear cell acanthoma (serpiginous arrangement) |
Vessel Arrangement Types
| Vessel Arrangement | Definition | Key Associations |
|---|---|---|
| Random | No specific arrangement pattern | Polymorphic linear vessels in melanoma |
| Clustered | Concentrated in certain areas | Various; may indicate focal pathology |
| Serpiginous | Dotted/coiled vessels in linear snakelike pattern | Clear cell acanthoma (pathognomonic) |
| Linear | Dotted/coiled vessels in straight lines | SCC in situ (flat component) |
| Centered | Vessels at center of skin-colored clods | Verruca, congenital nevus, seborrheic keratosis |
| Radial | Linear vessels from periphery toward center, not crossing | Radial arrangement of vessels |
| Reticular | Linear vessels crossing at right angles (net-like) | Sun-damaged skin, telangiectasia macularis perstans |
| Branched | Serpentine vessels dividing into thinner branches from main stem | BCC (arborizing vessels -- hallmark pattern) |
Monomorphous Patterns and Diagnoses
| Monomorphous Pattern | Diagnosis | Key Caveats |
|---|---|---|
| Clods-only (red/purple/blue) | Hemangioma | Small hemangiomas may have some linear vessels; vessels within clods = excise |
| Centered vessels (in skin-colored clods) | Verruca, congenital nevus, seborrheic keratosis | Clods must be skin-colored (not pink/red); white lines override this pattern |
| Serpiginous vessels only | Clear cell acanthoma | No differential diagnosis (pathognomonic) |
| Reticular vessels only | Benign (sun damage, telangiectasia macularis perstans) | Vessels of superficial horizontal vascular plexus made visible by dermal atrophy |
Polymorphous Patterns and Malignancy
| Vessel Pattern | Suspicion | Key Features |
|---|---|---|
| Dots + any linear vessels | Melanoma | Dots as a separate pattern (not scattered among linear); dots in macular areas, linear in raised areas |
| Branched serpentine (arborizing) | BCC | Translucent stroma casts vessels into sharp relief; monomorphous pattern |
| Polymorphous linear (looped, curved, serpentine, helical, coiled) | Melanoma (if not SK or dermal nevus) | Often in random arrangement; from distorted dermal papillae |
| Polymorphous (any combination) | Assess for biopsy | Also seen in SK and dermal nevi -- pattern recognition of benign entities is key |
6. Algorithm Flowchart
flowchart TD
A[Nonpigmented Lesion<br/>of Concern] --> B{Common Benign<br/>Entity?}
B -->|Yes| C[Benign -- No<br/>Further Action]
B -->|No / Red Flags| D{Step 1: Ulceration<br/>Present?}
D -->|Yes| E[Biopsy Recommended<br/>Most likely BCC]
D -->|No| F{Step 2: White<br/>Clues Present?}
F -->|White lines| G[Biopsy Recommended<br/>Most likely BCC]
F -->|Keratin clues<br/>on raised lesion| H[Biopsy Recommended<br/>Most likely SCC/KA]
F -->|No white clues| I{Step 3: Vessel<br/>Pattern Analysis}
I -->|Clods-only| J[Hemangioma]
I -->|Centered in<br/>skin-colored clods| K[Verruca / CN / SK]
I -->|Serpiginous only| L[Clear Cell<br/>Acanthoma]
I -->|Reticular only| M[Benign -- Sun<br/>Damage]
I -->|Other patterns| N{Polymorphous<br/>Assessment}
N -->|Dots + linear| O[Suspect Melanoma]
N -->|Branched serpentine<br/>+ translucent stroma| P[Suspect BCC]
N -->|Other polymorphous| Q[Biopsy -- Malignancy<br/>Not Excluded]
Text version of algorithm
NONPIGMENTED LESION OF CONCERN
(Brown/gray color absent; no melanin-based pigmentation)
|
v
[Can you identify this as one of the 6 common benign entities?]
(Nonpigmented nevus, benign keratinocytic lesion, hemangioma
dermatofibroma, sebaceous gland hyperplasia, cyst)
|
YES -+-> BENIGN -- No further action needed
| (Unless red flags are present)
NO --+
|
v
[Are RED FLAGS present?]
- Patient concern or evidence of change
- Clinical pattern-breaker
- EFG lesion (elevated, firm, growing)
- Ulceration visible clinically
- Surface keratin on raised lesion
- Polarizing-specific white lines on dermoscopy
|
YES -+-> Proceed to formal algorithm (below)
|
NO --+-> If still uncertain, proceed to formal algorithm
|
v
========================================
PREDICTION WITHOUT PIGMENT ALGORITHM
========================================
|
STEP 1: IS THERE ULCERATION?
(Clinical or dermatoscopic -- look for adherent fiber)
|
YES -+-> BIOPSY RECOMMENDED
| (Most likely BCC; also consider SCC, melanoma)
| Use vessels + other clues to predict specific Dx
|
NO --+
|
v
STEP 2: ARE WHITE CLUES PRESENT?
|
[A] White lines (any nonpigmented lesion)?
- Polarizing-specific: straight, perpendicular
non-crossing, shift with rotation
- Must be at least as white as perilesional skin
|
YES -+-> BIOPSY RECOMMENDED
| (Most likely BCC; also SCC in situ, LPLK
| amelanotic melanoma, DF, Spitz nevus)
| Polymorphous + dots --> think melanoma
|
NO --+
|
[B] Keratin clues (raised nonpigmented lesion only)?
- Surface keratin (clinical or dermatoscopic)
- White structureless areas (dermatoscopic)
- White circles (dermatoscopic) -- 87% specific for SCC/KA
|
YES -+-> BIOPSY RECOMMENDED
| (Most likely SCC / keratoacanthoma)
|
NO --+
|
v
STEP 3: VESSEL PATTERN ANALYSIS
(Only reached when no ulceration AND no white clues)
|
[Is the pattern one of the 4 benign monomorphous patterns?]
|
(a) Clods-only --> HEMANGIOMA (if stable; no vessels within clods)
(b) Centered vessels in skin-colored clods --> VERRUCA / CN / SK
(c) Serpiginous only --> CLEAR CELL ACANTHOMA (pathognomonic)
(d) Reticular only --> BENIGN (sun damage / mastocytosis)
|
YES -+-> BENIGN pattern -- monitor (with caveats above)
|
NO --+
|
v
[ALL OTHER VESSEL PATTERNS]
|
+-> ASSESS FOR BIOPSY
|
+-> Dots + linear vessels --> suspect MELANOMA
+-> Branched serpentine + translucent stroma --> suspect BCC
+-> Polymorphous linear (random) --> suspect MELANOMA
+-> Other polymorphous --> BIOPSY (malignancy not excluded)
7. Clinical Pearls
Adherent fiber is a subtle but powerful clue. A single adherent fiber on dermoscopy may be the only evidence of micro-ulceration in an early BCC. Always look for trapped material on the lesion surface.
White circles are the most specific keratin clue. At 87% specificity for SCC/KA, white circles can enable confident diagnosis of very small SCCs that would otherwise be impossible to diagnose at that size. This clue has been a game-changer for early SCC detection.
The hierarchy is strict: ulceration > white clues > vessels. If ulceration or white clues are present, do not rely on a benign vessel pattern to avoid biopsy. Vessels are supplementary evidence when higher-priority clues exist.
Skin-colored vs. pink clods -- a critical distinction. For the centered vessel pattern, the clods must be truly skin-colored. Some nodular melanomas can have vessels centered in pink clods. Beware of pressure artifact: pressing too hard on the dermatoscope can blanch pink clods to appear skin-colored. If you see pink clinically, trust the clinical finding.
Translucent stroma is the hallmark of BCC, not the vessels themselves. BCC's branched serpentine vessels may blend seamlessly with the surrounding dermal vascular plexus. What makes them diagnostic is the translucent (myxoid) stroma that casts them into sharp relief.
Dotted vessels in melanoma form a separate pattern, not scattered dots. A few dots among predominantly linear vessels is not a polymorphous pattern. In melanoma, the dotted vessel pattern usually appears as a distinct cluster or area, reflecting the macular (in situ) component of the tumor.
The serpiginous pattern is pathognomonic for clear cell acanthoma. It has no differential diagnosis. However, do not confuse the serpiginous arrangement (dotted/coiled vessels in a snakelike pattern) with the linear serpentine vessel type (individual snakelike vessels) -- these are different concepts.
"Look at thousands" is real advice, not hyperbole. The authors explicitly recommend examining thousands of obviously benign hemangiomas, seborrheic keratoses, and dermal nevi to internalize their protean morphology. This deliberate practice builds the pattern recognition that the algorithm complements.
EFG is an excision criterion independent of dermoscopy. Any elevated, firm, and continuously growing lesion should undergo excision biopsy regardless of what dermoscopy shows. This clinical red flag supersedes any benign dermatoscopic pattern.
Use all available information. Because nonpigmented lesions lack the rich dermoscopic landscape of pigmented lesions, both clinical and dermatoscopic findings should be integrated. Clinical context (patient age, anatomic site, history) is especially important.
9. Cross-References
| Topic | Reference |
|---|---|
| Prediction without Pigment algorithm and flowchart | Chapter 4c |
| Adherent fiber as clue to micro-ulceration | Chapter 4c |
| Polymorphous vessels in ulcerated BCC | Chapter 4c |
| Secondary keratinization in ulcerated BCC | Chapter 4c |
| Polarizing-specific white lines in BCC | Chapter 4c |
| Amelanotic melanoma with white lines | Chapter 4c |
| Dermal papilla vessel schematic and morphologies | Chapter 4c |
| Coiled vessels (SCC in situ) and looped vessels (invasive SCC) | Chapter 4c |
| Surface keratin and white structureless area in SCC | Chapter 4c |
| White circles in SCC (hand, scalp, ear) | Chapter 4c |
| Vessel structure types (8 types illustrated) | Chapter 4c |
| Vessel arrangement types (8 types illustrated) | Chapter 4c |
| Clods-only pattern in hemangioma | Chapter 4c |
| Centered vascular pattern in seborrheic keratosis | Chapter 4c |
| Serpiginous vascular pattern in clear cell acanthoma | Chapter 4c |
| Reticular vessel pattern on sun-damaged skin | Chapter 4c |
| Branched serpentine vessels with translucent stroma in BCC | Chapter 4c |
| White circles overriding vessel clues in SCC | Chapter 4c |
| Polymorphous vessels with dots in melanoma | Chapter 4c |
| Original publication | Rosendahl C et al. Dermatol Pract Concept. 2014;4(1):9 |
| SCC/KA dermoscopy and white circles | Rosendahl C et al. Arch Dermatol. 2012 |
| EFG criteria for nodular melanoma | Chamberlain AJ et al. J Am Acad Dermatol. 2003;48:694-701 |
| Chaos and Clues for pigmented lesions | Chapter 5a (Module 06) |
| Pattern analysis fundamentals | Chapter 4a (Module 03) |
10. Related Modules
| Module | Relationship |
|---|---|
| Module 01: Introduction and Principles | Prerequisite -- polarized vs. nonpolarized dermoscopy critical for identifying white lines |
| Module 02: Histopathologic Correlations | Prerequisite -- understanding vessel-histopathology correlations and white structure correlates |
| Module 03: Pattern Analysis Revised | Prerequisite -- foundational vocabulary of structures, patterns, and colors used throughout this algorithm |
| Module 04: Top-Down 2-Step Algorithm | Parallel algorithm -- alternative approach to equivocal lesion analysis |
| Module 06: Chaos and Clues | Companion algorithm -- the pigmented-lesion counterpart to Prediction without Pigment |
| Module 09: Basal Cell Carcinoma | Deep dive -- arborizing vessels, ulceration, translucent stroma, and BCC-specific features |
| Module 11: SCC Spectrum | Deep dive -- keratin patterns, coiled/looped vessels, white circles in SCC and KA |
| Module 13: Vascular Lesions | Deep dive -- hemangioma morphology, clods-only pattern, vascular differential diagnoses |
| Module 14: Adnexal Neoplasms | Deep dive -- clear cell acanthoma and its pathognomonic serpiginous vessel pattern |
| Module 26: Amelanotic and Hypomelanotic Melanoma | Deep dive -- polymorphous vessels, dotted vessel patterns, and melanoma-specific vascular clues |
This module is part of the Dermoscopy Educational Course. It is intended for educational purposes and should be used alongside the referenced figures for complete visual understanding of the described dermoscopic features.
Image Sources & Citations
- DERM12345 (Skin Lesion Dataset with 40 Subclasses): DERM12345: A Large-scale Skin Lesion Image Dataset with 40 Subclasses. Figshare. 2023. License: CC-BY-4.0.
- HIBA Dermoscopy Dataset: HIBA Dermoscopy Dataset. Hospital Italiano de Buenos Aires. License: CC-BY-4.0.