Module 02: Histopathologic Correlations of Dermoscopic Structures
Source: Dermoscopy Educational Course Authors: Morgado-Carrasco D, Riquelme-Mc Loughlin C, Braun RP, Yelamos O
1. Learning Objectives
After completing this module, the learner should be able to:
- Explain the relationship between melanin depth within the skin and the color observed on dermoscopy (black, brown, gray, blue) and identify the corresponding epidermal or dermal layer for each color.
- Identify the histopathologic correlate of at least 12 major dermoscopic structures seen in melanocytic neoplasms, including pigmented network, negative network, angulated lines, globules, dots, streaks, homogeneous blue pattern, blotches, regression structures, shiny white structures, and blue-whitish veil.
- Differentiate typical from atypical variants of dermoscopic structures (e.g., typical vs. atypical pigment network; regular vs. irregular blotches) and state the diagnostic significance of each variant.
- Describe the unique microanatomic features of special sites (face, volar skin, mucosa, nails) that give rise to site-specific dermoscopic patterns, and name the histopathologic correlate of each pattern.
- List the specific dermoscopic structures associated with each major nonmelanocytic neoplasm (BCC, keratinizing tumors, SK, angioma/angiokeratoma, dermatofibroma, LPLK, clear cell acanthoma, sebaceous neoplasms, and porokeratosis) and state their histologic basis.
- Recognize the dermoscopic hallmarks and their histologic correlates in inflammatory dermatoses (psoriasis, dermatitis, lichen planus, rosacea, granulomatous diseases) and infectious conditions (molluscum contagiosum, warts, scabies).
- Identify at least seven trichoscopic structures (yellow dots, black dots, pinpoint white dots, white patches, blue-gray dots, empty follicles, peripilar casts) and correlate each with its histopathologic finding and associated disorder.
- Apply knowledge of dermoscopic-histopathologic correlations to predict histologic subtype, Breslow thickness, and potential genetic mutations in melanoma based on dermoscopic features.
2. Prerequisites
- Module 01: Introduction & Principles of Dermoscopy -- Understanding of polarized vs. nonpolarized dermoscopy, basic equipment operation, and fundamental image capture principles is essential before studying histopathologic correlates.
3. Key Concepts
3.1 What Is Histopathologic-Dermoscopic Correlation?
Dermoscopy provides a horizontal (en face) view of skin lesions, enabling visualization of epidermal and superficial dermal structures that are invisible to the naked eye. Since dermoscopy uses magnification with a polarized and/or nonpolarized light source, the structures observed correspond to specific histopathologic findings visible on microscopic examination. This relationship between what is seen under the dermatoscope and what is seen under the microscope constitutes the histopathologic-dermoscopic correlation.
3.2 Why Correlations Matter
- Diagnostic bridge: Dermoscopy is the link between clinical examination and histopathology; most structures observed under dermoscopy have a direct histopathological correlate.
- Guided biopsy: Knowledge of correlations allows clinicians to select the most informative area within a large or complex lesion for biopsy.
- Ex vivo dermoscopy: Dermoscopy can be performed on formalin-fixed specimens, providing the pathologist with a lesion overview before tissue processing and guiding step-sectioning.
- Prognostic value: Certain dermoscopic structures predict Breslow thickness, mitotic activity, sentinel lymph node positivity, and genetic mutations.
- Treatment guidance: Dermoscopic patterns can predict histologic subtypes of BCC and SCC, informing treatment planning.
3.3 The Role of Chromophores
The colors observed on dermoscopy are produced by the interaction of light with skin chromophores -- endogenous substances that absorb and reflect light at specific wavelengths. The principal chromophores are:
| Chromophore | Color(s) Produced | Key Determinants |
|---|---|---|
| Melanin | Black, brown, gray, blue | Amount and depth within the skin |
| Hemoglobin / Blood | Red, dark red, blue-black | Oxygenation, vascular volume, thrombosis |
| Keratin | Yellow, brown | Thickness and composition of cornified layer |
| Collagen | White | Fibrosis, sclerosis, stromal alteration |
| Lipids / Sebum | Yellow, orange | Sebaceous differentiation, xanthomization |
| Serum / Lymph | Orange, yellow | Erosions, superficial ulcerations |
4. Core Content
4.1 Colors in Dermoscopy

The spectrum of colors visible under dermoscopy is determined by the quantity and location of chromophores within the skin. Understanding these color-depth relationships is foundational to interpreting every dermoscopic structure.
4.1.1 Melanin and Depth
Melanin is the most important chromophore in dermoscopy. Its color changes predictably with depth:
| Location of Melanin | Color Under Dermoscopy |
|---|---|
| Stratum corneum / upper epidermis | Black |
| Mid- to low epidermis / dermo-epidermal junction (DEJ) | Brown |
| Papillary dermis | Gray |
| Deeper dermis (reticular dermis) | Blue or blue-gray |
| Multiple layers simultaneously | Black (dark, confluent) |
When melanin is present in the stratum corneum or upper epidermis, it appears black because it is closest to the light source and absorbs light before significant scattering occurs. As melanin moves deeper into the skin, increasing scatter by dermal collagen shifts the perceived color toward gray and blue according to the Tyndall effect.
4.1.2 Hemoglobin and Blood
- Red/pink hues: Blood vessels and vascular volume in the superficial dermis.
- Dark red to brown-red: Hemorrhagic crusts on erosions or ulcerations.
- Jet black: Congealed blood (e.g., thrombosed vascular spaces in angiomas).
- Blue-black lacunae: Partially or completely thrombosed dermal vessels.
4.1.3 Keratin
- Yellow to brown: Stratum corneum, devoid of blood and melanin, appears yellow. Hyperkeratosis and parakeratosis produce opaque yellow-brown structures (scale).
- Areas with sebaceous differentiation also manifest a yellow hue.
4.1.4 Collagen
- White color: Depigmentation, fibrosis, alterations in the collagen matrix, or keratin within cysts produce white structures.
4.1.5 Lipids, Serum, and Other Substances
- Yellow to orange: Lipids, lymph, and keratin produce yellow-orange colors. Cell xanthomization is associated with homogeneous yellow-orange areas.
- Orange hues: Serum present in erosions or superficial ulcerations.
4.1.6 Specific Color-Structure Associations
Certain colors, when linked to specific dermoscopic structures, have important histopathologic correlates:
- White globules are associated with balloon cell changes in nevi.
- Homogeneous yellow-orange areas are linked to cell xanthomization.
- Black lacunae are associated with thrombosed vascular spaces in angiomas.
Check Your Understanding
What determines the color of melanin as seen through the dermatoscope, and how does depth affect color?
The color depends on the depth of melanin in the skin. Melanin in the stratum corneum appears black, in the basal layer it appears brown, in the papillary dermis it appears gray-blue, and in the reticular dermis it appears steel-blue. Deeper melanin scatters longer wavelengths preferentially, shifting the perceived color.
4.2 Melanocytic Neoplasm Correlates
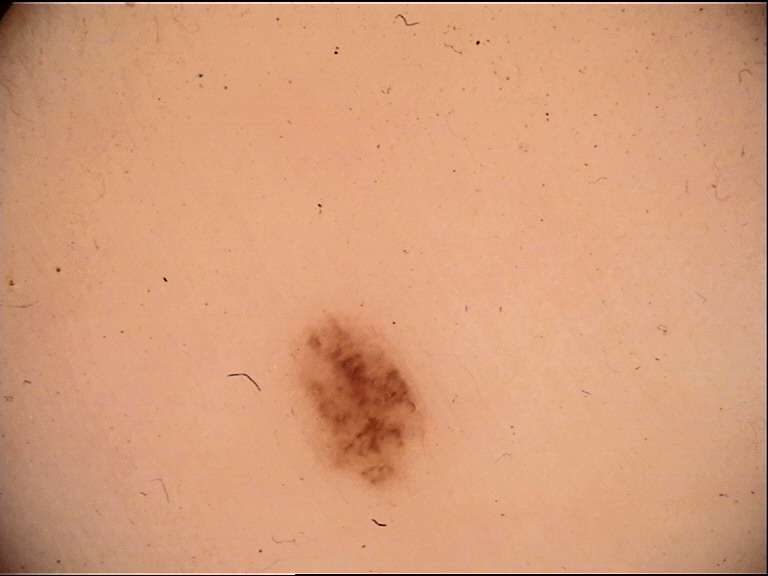
4.2.1 Pigmented Network
Dermoscopic appearance: Intersecting brown lines creating a reticular grid-like or fishnet-like pattern with hypopigmented "holes."
Histopathologic correlate: The lines correspond to melanin within keratinocytes and melanocytes along the rete ridges. The holes of the network correspond to the suprapapillary plates (the tips of the dermal papillae and the overlying thinner epidermis). The width of the network lines reflects the width of the rete ridges.
Typical (regular) pigment network:
- Lines have minimal variation in width and color.
- Hallmark of benign melanocytic nevi with a junctional component.
- Histologically: regular, uniform rete ridges.
- Can also appear in nonmelanocytic lesions: ink-spot lentigo, dermatofibroma, accessory (supernumerary) nipple.
Atypical pigment network:
- Irregularly meshed; increased variability in thickness, color (especially gray), and distribution.
- Associated with dysplastic nevi and superficial spreading melanoma.
- Histologically: disarrangement of rete ridges, confluence of melanocytic nests, and changes in melanin distribution within the epithelium.
Pseudonetwork (facial skin): Pigment network is usually absent on the face due to a normally flattened DEJ. Instead, brown structureless areas interrupted by hypopigmented follicular openings create a pseudonetwork pattern. Also uncommon on palms/soles, where dermatoglyphics produce parallel pigment patterns instead.
4.2.2 Negative Network
Dermoscopic appearance: Elongated to curvilinear brown globular structures with relative hypopigmentation surrounding them. The hypopigmented areas take on the appearance of serpiginous lighter "lines" surrounding hyperpigmented globular structures.
Histopathologic correlate: The hypopigmented lines correlate with broadened epidermal rete ridges, which often contain overlying surface dells and wedge-shaped hypergranulosis. The pigmented globules correlate with predominantly junctional proliferation of melanocytes along and between elongated rete ridges. A negative network-like appearance is also seen when there is bridging of adjacent rete ridges, or when large melanocytic nests are present within widened dermal papillae straddled by thin elongated rete ridges.
Clinical associations: Most commonly melanoma (especially melanomas arising in nevi) and Spitz nevi. Occasionally seen in small congenital-type nevi.
Important distinctions:
- Negative network is visible with both polarized and nonpolarized light.
- Should not be confused with a grid-like pattern created by intersecting shiny white lines (polarized light only), which represent collagen (seen in melanoma, Spitz nevi, dermatofibromas).
- Reticular depigmentation can resemble a negative network; most often seen in fibroepithelioma of Pinkus (a BCC subtype), likely representing intersecting basaloid cords. Visible with both polarized and nonpolarized light but more conspicuous with polarized light.
4.2.3 Angulated Lines
Dermoscopic appearance: Brown to brownish-gray dots coalescing to form lines that intersect at acute angles, creating a zig-zag pattern. These can further coalesce to create polygonal shapes such as rhomboids.
Histopathologic correlate: The lines correspond to a constellation of findings including a flat DEJ, single-cell proliferation of melanocytes along the DEJ with or without pagetoid spread, and the presence of melanophages in the superficial dermis. Confocal microscopy suggests the angulated nature may correspond to pagetoid spread of melanoma cells within the interfollicular epidermis extending from one follicle to the next.
Clinical associations: Lentigo maligna (LM) on the head/neck area and lentiginous melanomas on chronically sun-damaged skin. Angulated lines forming polygons in nonfacial locations tend to be larger than the rhomboids of facial LM.
4.2.4 Globules
Dermoscopic appearance: Round to oval, well-demarcated structures larger than 0.1 mm in diameter. Usually aggregated or at the periphery of a melanocytic lesion.
Histopathologic correlate by color:
| Globule Color | Histologic Correlate |
|---|---|
| Brown or black | Nests of melanocytes at the epidermis or DEJ |
| Blue | Melanocytic nests in the dermis |
| White | Melanocytes displaying balloon cell changes |
| Blue-gray (in BCC) | Melanin/melanocyte-containing basal cell tumor islands |
Clinical significance of distribution:
- Peripheral globules: Indicative of horizontal growth (nevus or superficial spreading melanoma).
- In melanoma: Globules vary in size, shape, and color; frequently found focally and randomly distributed at the periphery.
- Focal eccentric cluster of globules at the periphery of a raised homogeneous lesion: Suspect a BAP1-inactivated melanocytic tumor (BIMT) or "bapoma." Histology reveals a biphasic cell population -- a banal-appearing dermal population (globular component) and a spitzoid population with loss of BAP1 expression (homogeneous area). Multiple BIMTs are associated with a cancer syndrome (uveal melanoma, cutaneous melanoma, mesothelioma, renal cell carcinoma).
4.2.5 Dots
Dermoscopic appearance: Small, round, well-circumscribed structures smaller than 0.1 mm in diameter (similar to the diameter of a terminal hair follicle).
Histopathologic correlate by color:
| Dot Color | Histologic Correlate |
|---|---|
| Black | Melanin in the upper epidermis or stratum corneum |
| Brown | Small melanocytic nests in the epidermis or DEJ |
| Blue-gray | Melanin in the upper dermis or within dermal melanophages (e.g., peppering/granularity, regression) |
| Red | Vessels (cutaneous tumors and inflammatory conditions) |
Distribution patterns and significance:
- In nevi: Usually associated with a typical network; clustered in the center, on top of network lines, or in the holes of the network.
- In melanoma: Distributed in a disorganized manner; may be found focally at the periphery; often not associated with a network or associated with an atypical network.
- In BCC: Blue-gray and brown dots distributed in a random, birdshot scatter pattern, corresponding to small aggregates of pigmented superficial BCC cells.
Clinical Scenario
A 45-year-old woman presents with a 7 mm brown macule on the right calf. Dermoscopy reveals a reticular pattern of brown lines forming a meshwork with hypopigmented holes. The lines are relatively uniform in thickness and color. At the periphery, multiple small round brown structures (approximately 0.1 mm diameter) are clustered symmetrically.
What is your diagnosis and key dermoscopic findings?
Compound melanocytic nevus
The reticular pattern represents a typical pigment network, where the brown lines correspond histopathologically to melanin within keratinocytes and melanocytes along the rete ridges, and the hypopigmented holes correspond to the suprapapillary plates. The uniform width and color of the lines indicates regular rete ridges (benign). The peripheral brown globules correspond to nests of melanocytes at the DEJ, indicating active horizontal growth typical of a compound nevus.
4.2.6 Streaks
Dermoscopic appearance: Linear pigmented projections located at the periphery of lesions, projecting from the tumor and radiating outward toward normal skin. The term encompasses both radial streaming (linear extensions without a bulbous ending) and pseudopods (linear projections with a bulbous terminal ending).
Histopathologic correlate: Linearly confluent junctional nests of pigmented melanocytes at the periphery of the lesion.
Clinical significance of distribution:
- Symmetrical distribution of streaks around the entire perimeter: Favors Reed's nevus.
- Asymmetrical or focal distribution at the periphery: Favors superficial spreading melanoma.
Association: Streaks indicate the radial growth phase in both Reed's nevi and superficial spreading melanomas.
4.2.7 Homogeneous Blue Pattern
Dermoscopic appearance: Blue color with the absence of other dermoscopic structures throughout the entire lesion when viewed with nonpolarized light. When viewed with polarized light, shiny white lines may occasionally be visible.
Histopathologic correlate: Densely pigmented melanocytes or melanophages in the dermis.
Differential diagnosis: Blue nevi, areas of extensive regression, pigmented nodular melanoma, epidermotropic metastatic melanoma, nodular pigmented BCC, and radiation tattoos.
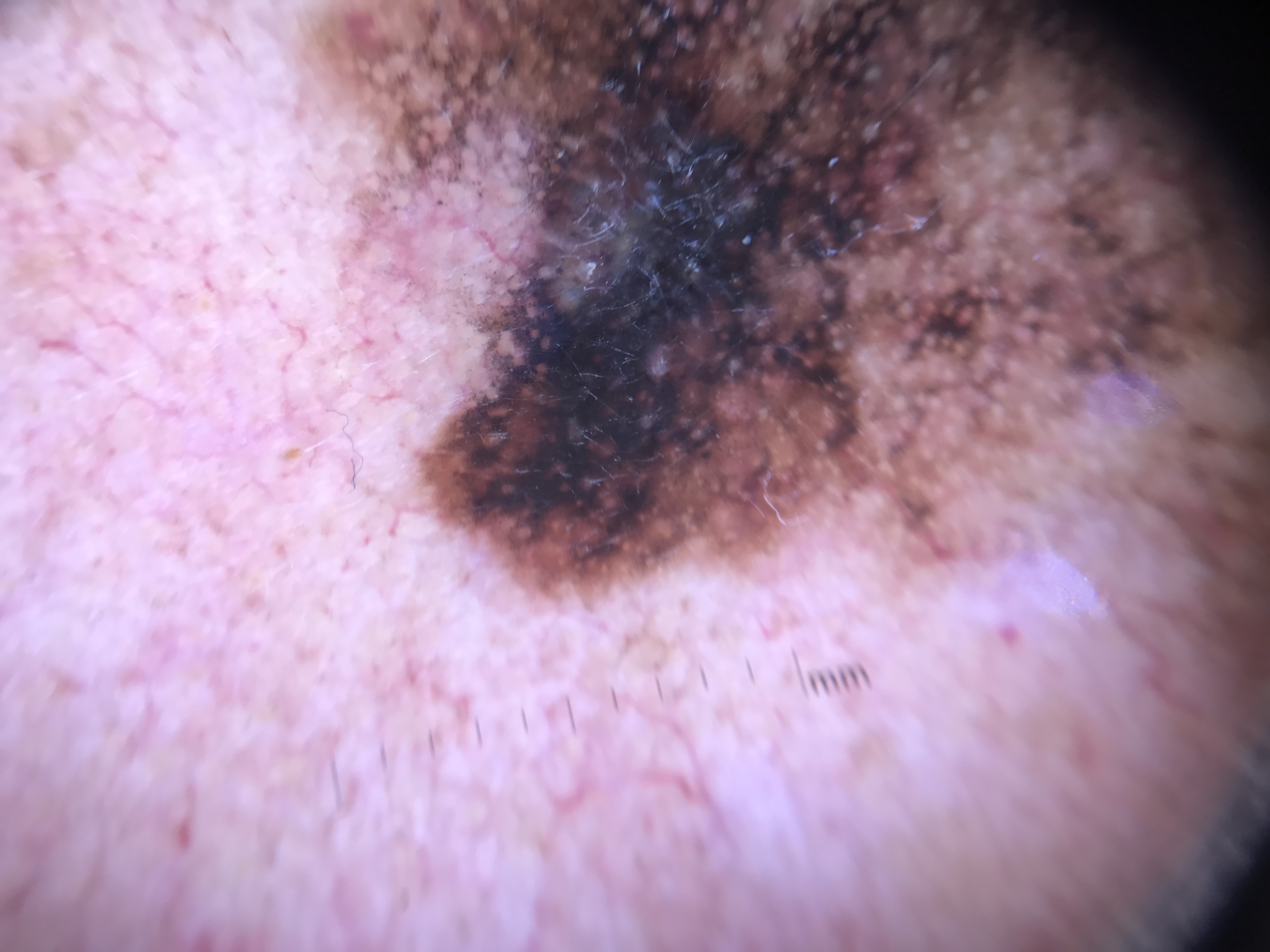
4.2.8 Blotches
Dermoscopic appearance: Heavily pigmented dark brown to black structureless areas occupying more than 10% of the lesion's surface area, precluding visualization of any other structure.
Histopathologic correlate: Abundant melanin in one or more layers of the epidermis, with or without pigment in the underlying dermis.
Variants:
| Blotch Type | Features | Clinical Association |
|---|---|---|
| Regular blotch | Isolated, symmetric, homogeneous, centrally located | Melanocytic nevi (with reticular periphery) |
| Irregular blotch | Asymmetric, heterogeneous, off-centered; or multiple blotches | Melanoma, dysplastic nevi |
| Black lamella | Excessive melanin in the stratum corneum; transient | Nevi after UV exposure |
Black lamella: A specific type of blotch caused by excessive melanin accumulation in the stratum corneum. This is transient (appearing after ultraviolet exposure) and can be removed by tape-stripping the upper stratum corneum layers, revealing the underlying dermoscopic structures. Black lamella typically reappears 3-12 months after tape stripping. Blotches caused by melanin below the stratum corneum cannot be tape-stripped away.
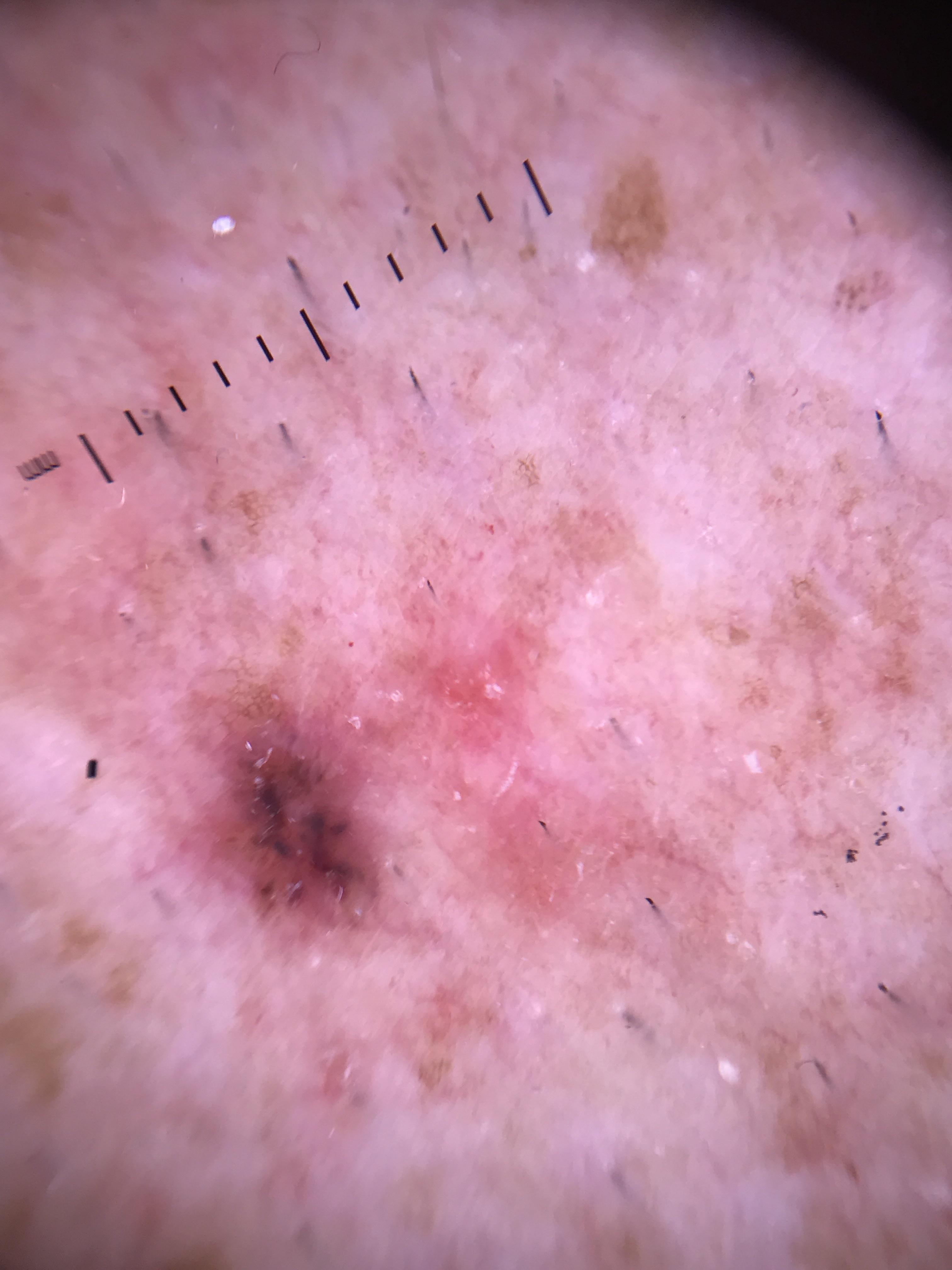
4.2.9 Regression Structures: Granularity/Peppering and Scarlike Depigmentation
Regression structures encompass two dermoscopic features that can occur together or independently. Both are flat and nonpalpable.
Granularity (peppering):
- Dermoscopic appearance: Multiple tiny gray dots.
- Histopathologic correlate: Free melanin in the dermis or within melanophages.
- Clinical associations: Regression areas within melanoma, lichen planus-like keratosis (LPLK), and occasionally melanocytic nevi.
Scarlike depigmentation (scarlike areas):
- Dermoscopic appearance: White structureless areas lighter than the surrounding perilesional skin, often porcelain-white in color. In melanocytic lesions, these areas typically do not display shiny white lines or vessels.
- Histopathologic correlate: Dermal fibrosis.
- Note: Sectioning through the scarlike area often reveals nondiagnostic features histologically.
4.2.10 Shiny White Structures (SWS)
Formerly known as crystalline structures and chrysalis, SWS are only seen with polarized dermoscopy. Three morphologies have been described:
1. Shiny white lines:
- Dermoscopic appearance: Short white lines oriented parallel or orthogonal to each other. They display angular dependence (conspicuity changes as the dermatoscope is rotated). When multiple lines intersect, they create square-shaped structures that can appear as a white grid-like pattern.
- Histopathologic correlate: Presumed to correspond to birefringent collagen bundles, thought to be altered or new collagen resulting from the tumor's influence on fibroblasts and/or stroma.
- Clinical associations: Melanoma, Spitz nevi, LPLK, dermatofibroma. In melanomas, their presence is often associated with dermal invasion.
- Important: The grid-like pattern should not be confused with a negative network or reticular depigmentation, neither of which displays angular dependence.
2. Shiny white blotches and strands:
- Dermoscopic appearance: Blotches are white homogeneous clods; strands are parallel, linear white areas that are usually longer than shiny white lines and do not intersect at orthogonal angles.
- Histopathologic correlate: Strands correspond to stromal alteration. Blotches may represent stromal alteration around BCC tumor islands or collections of mucin.
- Clinical associations: Highly specific for BCC (combined presence of blotches and strands).
3. Rosettes:
- Dermoscopic appearance: Four bright white dots or clods arranged as a four-leaf clover or square (only visible with polarized light).
- Histopathologic correlate: Hyperkeratosis of the follicular opening. Smaller rosettes correspond to concentric horn material in adnexal openings (follicular or eccrine ducts); larger rosettes correspond to concentric perifollicular fibrosis.
- Clinical associations: Multiple rosettes are common in actinically damaged skin, AK, and SCC. Isolated rosettes can be seen in BCC, melanoma, and inflammatory/infectious dermatoses.
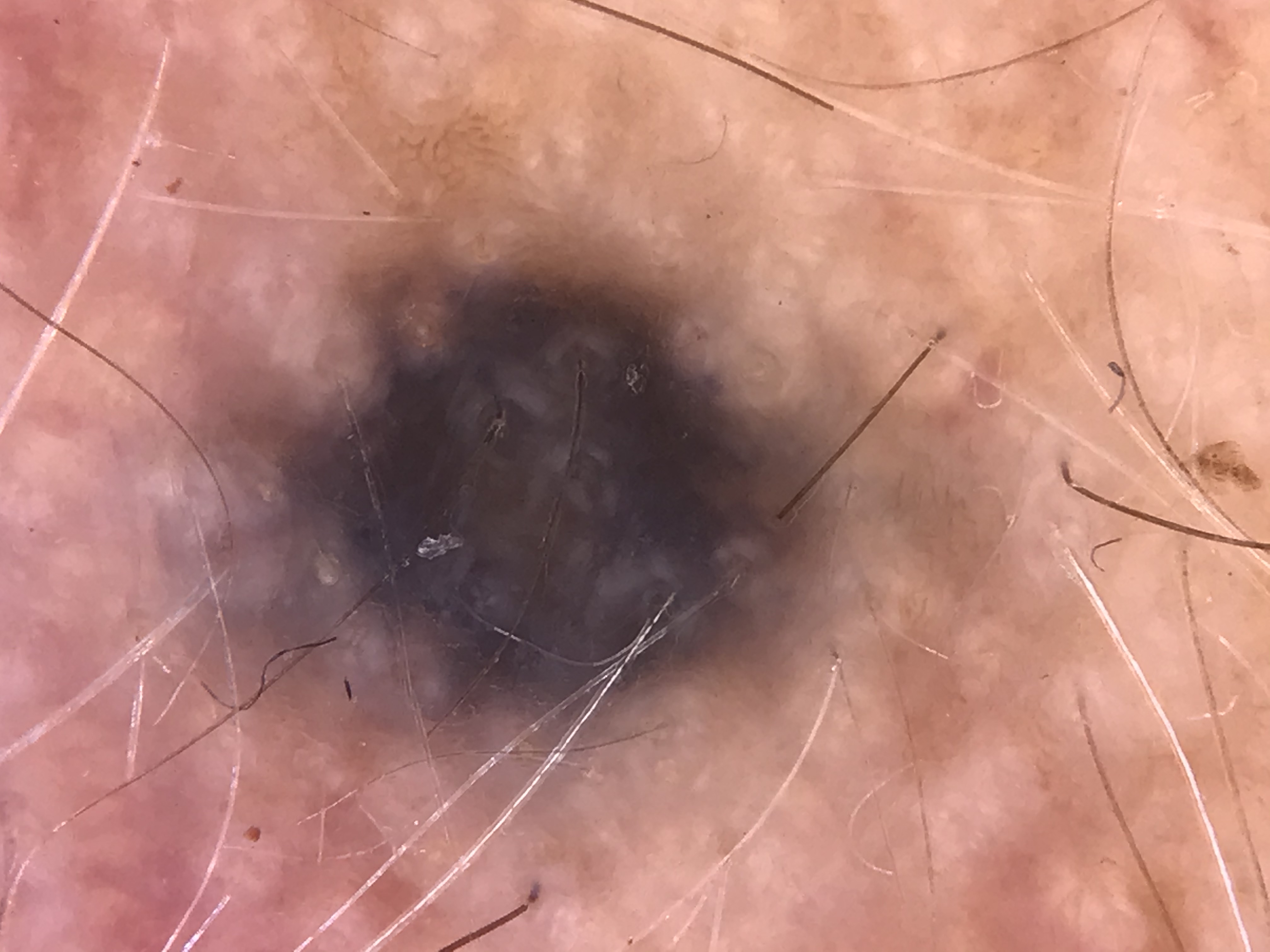
4.2.11 Blue-Whitish Veil (BWV)
Dermoscopic appearance: A structureless blue area with an overlying white "ground-glass" haze. Clinically, the BWV corresponds to the raised/palpable areas of a pigmented lesion.
Histopathologic correlate: Heavily pigmented melanocytes in the dermis in combination with acanthosis and compact orthokeratosis.
Clinical associations: Most often melanoma; also Reed's nevi. A BWV-like appearance can occasionally be seen in heavily pigmented nodular BCC or heavily pigmented SK (melanoacanthoma), but in pigmented SKs, the BWV is almost never structureless -- it is typically studded with comedo-like openings and milia-like cysts.
Check Your Understanding
What is the histopathologic correlate of a pigment network seen on dermoscopy?
The pigment network corresponds to melanin along the rete ridges at the dermal-epidermal junction. The lines of the network correspond to pigmented rete ridges, and the holes correspond to the dermal papillae.
Key Takeaways
- Melanin color changes predictably with depth: black (superficial epidermis), brown (DEJ), gray (papillary dermis), blue (reticular dermis).
- Typical pigment network has uniform lines corresponding to regular rete ridges, while atypical network with variable thickness and gray color suggests dysplasia or melanoma.
- Peripheral globules indicate horizontal growth; asymmetric focal globules suggest melanoma while symmetric peripheral globules favor a growing nevus.
- Shiny white structures are visible only under polarized dermoscopy and include lines (collagen), blotches/strands (BCC-specific), and rosettes (keratinized adnexal openings).
4.3 Special Site Correlates
The microanatomy of the rete ridge pattern at special sites (face, volar skin, mucosa, nails) differs from that of nonglabrous skin, resulting in unique dermoscopic patterns at each site.
4.3.1 Facial Skin
Microanatomic features: Thin epidermis with thin stratum corneum, relatively flat DEJ, and multiple pilosebaceous units.
Pseudonetwork pattern: Brown structureless/homogeneous pigmented areas interrupted by hypopigmented holes corresponding to adnexal openings. Histologically, this corresponds to pigmented cells/melanin in the epidermis with a flattened DEJ interrupted by adnexal/follicular openings.
Lentigo maligna (LM) progression features:
| Feature | Dermoscopic Appearance | Histopathologic Correlate | Stage |
|---|---|---|---|
| Gray dots (perifollicular) | Tiny gray-brown dots around follicular openings | Free melanin in dermis or within melanophages | Early (annular-granular pattern) |
| Brown dots (perifollicular) | Small brown dots around follicles | Small aggregates/nests of melanocytes | Early |
| Asymmetric pigmented follicular openings | Pigmentation around only part of the follicle (incomplete circles) | Melanocytes extending focally down one portion of the hair follicle | Early |
| Gray circles | Gray rings around follicles | Junctional proliferation of atypical melanocytes with varying follicular/dermal invasion | Early-intermediate |
| Concentric circles (circle within circle / isobar) | Circle within a circle around follicles | Increased melanocytes in follicular epithelium plus pigmentation in a rete ridge surrounding the follicle | Intermediate |
| Target-like pattern | Dot within a circle | Same as above | Intermediate |
| Pigmented follicular extensions | Fine pigment extensions from follicles (best seen at magnification) | Melanocyte proliferation along follicular epithelium | Intermediate |
| Angulated lines / rhomboids | Brown-gray lines intersecting at acute angles forming polygons | Flat DEJ, pagetoid spread of melanoma, melanophages in dermis | Intermediate-late |
| Blotches with preserved follicles | Dark areas with follicular openings still visible | Dense melanocyte proliferation with preserved follicular architecture | Late |
| Blotches with obliterated follicles | Solid dark areas, follicles no longer visible | Advanced melanocyte proliferation with follicular destruction | Late (advanced) |
4.3.2 Volar Skin
Microanatomic features: Thick cornified layer, dermatoglyphics (ridges and furrows), absence of hair follicles. Two distinct rete ridge systems exist: the crista limitans (corresponding to the dermatoglyphic furrows) and the crista profunda intermedia (corresponding to the ridges).
Parallel furrow pattern (benign):
- Dermoscopic appearance: Thin parallel pigmented lines in the furrows.
- Histopathologic correlate: Nevomelanocytes located in the crista limitans rete ridges, which correspond to the dermatoglyphic furrows (sulcus superficialis). These melanocytes transfer pigment to overlying keratinocytes.
- Association: Benign melanocytic lesions.
Parallel ridge pattern (malignant):
- Dermoscopic appearance: Thick parallel pigmented lines on the ridges.
- Histopathologic correlate: Melanocyte proliferation around the rete ridges associated with the acrosyringia (crista profunda intermedia). The melanoma is believed to arise from stem cells residing around the eccrine ducts.
- Association: Acral melanoma.
Lattice-like pattern (benign variant):
- Dermoscopic appearance: Parallel pigmented lines in the furrows plus pigmented lines crossing the ridges connecting one furrow to another.
- Histopathologic correlate: Anatomical variant of the parallel furrow pattern.
- Association: Commonly seen in nevi on the arch of the foot.
Fibrillar pattern:
- Dermoscopic appearance: Pigmented lines oriented diagonally across both furrows and ridges, all oriented in the same tangential direction.
- Histopathologic correlate: Vertically oriented epidermal melanin pigment columns angle in the direction of mechanical frictional forces as they enter the thickened stratum corneum.
- Association: Can be seen in both nevi and melanomas on weight-bearing or friction-exposed volar surfaces. Applying the dermatoscope at an angle or applying counter-pressure may reveal whether the pattern arises from furrows or ridges.
4.3.3 Mucosal Sites
Microanatomic features: Usually lacks a corneal layer. Rete ridge pattern may be attenuated, widened, or thin.
Benign mucosal melanocytic patterns:
| Pattern | Dermoscopic Appearance | Histopathologic Correlate |
|---|---|---|
| Homogeneous pattern | Structureless brown areas | Flattened rete ridges with acanthosis |
| Ring-like pattern | Pigmented circles | Hyperpigmented widened rete ridges with skip areas of pigmentation at top of narrow dermal papillae |
| Fish scale-like pattern | Half circles (variant of ring-like) | Same as ring-like pattern |
| Parallel / reticular-like pattern | Brown linear to slightly curved lines | Hyperpigmentation at the tip of obliquely elongated rete |
| Hyphal pattern | Nonlinear lines resembling fungal hyphae | Same as parallel pattern |
| Dotted-globular pattern | Multiple dots/globules of similar size and shape | Locally aggregated melanin in the upper dermis (lamina propria) |
Mucosal melanoma: A multicomponent pattern consisting of blue, gray, and white colors; regression structures; BWV; and structureless areas. Early-stage vulvar melanomas most often reveal structureless areas, gray globules and areas, blue and white structures, and red areas with irregular black-brown dots. Histologic correlation is similar to nonmucosal melanoma.
4.3.4 Nails
Melanonychia striata presents as a longitudinal pigmented band in the nail plate. The source of pigment is typically the nail matrix (below the cuticle and nail plate).
Key distinction -- activation vs. proliferation:
| Feature | Melanocytic Activation | Melanocytic Proliferation |
|---|---|---|
| Causes | Lentigo, drug-induced, post-inflammatory | Nevus, melanocytic hyperplasia, melanoma |
| Band appearance | Homogeneous gray band with gray granules and faint/no striations | Brown-black band with multiple linear striations and fine brown-black granules |
| Histology | Epithelial hyperpigmentation with normal melanocyte density | Increased melanocyte density |
Signs suggestive of nail apparatus melanoma (NAM):
- Irregular pigmented band with multiple colors
- Variable thickness of striated lines
- Loss of parallelism of striated lines
- Histologically: chaotic melanoma growth in the matrix
Micro-Hutchinson's sign: Periungual skin pigmentation (pigmentation of the cuticle) visible primarily with dermoscopy. Associated with NAM in adults. Important: a negative biopsy of the cuticle cannot exclude melanoma in the matrix.
Free edge dermoscopy -- locating the melanocytic source:
- Pigmentation in the upper part of the nail's free edge: melanocytic proliferation in the proximal nail matrix (produces top surface keratin).
- Pigmentation in the lower part of the nail's free edge: melanocytic proliferation in the distal nail matrix (produces undersurface keratin).
Direct nail matrix dermoscopy (intraoperative, 4 patterns):
| Pattern | Appearance | Histopathologic Correlate |
|---|---|---|
| Regular gray pattern | Fine regular grayish lines | Pigmentation in basal layer (melanocytic activation); no hyperplasia or nesting |
| Regular brown pattern | Regular brown lines | Benign melanocytic hyperplasia; no melanocytic nests |
| Regular brown with dots/globules/blotches | Regular brown lines + dots/globules/blotches of regular size/distribution | Melanocytic nevi; globules = nevus nests; blotches = focal melanin concentration |
| Irregular pattern | Irregular color/thickness lines +/- irregular dots/globules/blotches | Disorganized proliferation of atypical melanocytes; irregular nests. High sensitivity and specificity for melanoma |
Key Takeaways
- Facial skin lacks a true pigment network due to a flattened DEJ; instead, a pseudonetwork of brown areas interrupted by follicular openings is seen.
- On volar skin, parallel furrow pattern (pigment in furrows) indicates benign lesions while parallel ridge pattern (pigment on ridges) is the hallmark of acral melanoma.
- Nail melanonychia requires distinguishing melanocytic activation (homogeneous gray band) from proliferation (brown-black band with striations), with irregular bands and micro-Hutchinson sign raising concern for melanoma.
4.4 Nonmelanocytic Neoplasm Correlates
Clinical Scenario
A 68-year-old man presents with a slowly enlarging pigmented macule on the left cheek. Dermoscopy shows a brown structureless area interrupted by hypopigmented round openings (follicular ostia). Around several follicles, you observe tiny gray-brown dots forming incomplete circles. In one area, you see brown-gray lines intersecting at acute angles forming small polygon shapes.
What is your diagnosis and key dermoscopic findings?
Lentigo maligna (melanoma in situ on facial skin)
This case demonstrates the special site correlates of facial skin. The brown structureless area with hypopigmented follicular openings represents a pseudonetwork, which occurs because the normally flattened DEJ on the face prevents formation of a true pigment network. The perifollicular gray-brown dots forming incomplete circles (asymmetric pigmented follicular openings) indicate melanocytes extending focally down one portion of the hair follicle -- an early sign of lentigo maligna. The angulated lines forming rhomboids correspond to pagetoid spread of melanoma cells within the interfollicular epidermis, representing an intermediate-to-late stage feature. Biopsy is warranted.
4.4.1 Basal Cell Carcinoma (BCC)
Leaf-like areas:
- Brown to blue-gray linear to bulbous projections connected radially to an off-center base.
- Histologically: aggregates of pigmented BCC nests at the DEJ and papillary dermis.
- Associated with the superficial component of BCCs.
- Diagnostic of pigmented BCC in the absence of a pigment network.
Spoke wheel areas:
- Variant of leaf-like areas where radial projections converge toward a central darker hub.
- Histologically: pigmented BCC nests and cords connecting at the DEJ and upper dermis.
- Associated with superficial BCC.
Concentric globular structures:
- When individual spokes of spoke wheel areas are not discernible; dark globules inside lighter-colored globules (clod within a clod).
- Histologically: same as spoke wheel areas.
Blue-gray ovoid nests:
- Well-circumscribed blue-gray oval clods occupying at least 10% of the BCC surface area.
- Histologically: large, pigmented BCC tumor nodules in the dermis (pigmented nodular BCC).
- Suggestive of nodular growth pattern.
Multiple blue-gray globules:
- Larger than dots but smaller than ovoid nests; usually nonaggregated.
- Histologically: pigmented BCC tumor aggregates in the dermis.
- Suggestive of nodular BCC.
Blue-gray dots (in BCC):
- Pinpoint structures in a buckshot scatter pattern.
- Histologically: small BCC aggregates at the DEJ and/or papillary dermis.
- Associated with superficial BCC.
Ulcerations and erosions:
- Ulcerations: loss of entire epidermis; structureless red-orange color, often covered with serous or hemorrhagic crust. Indicative of nodular BCC.
- Erosions: partial loss of epidermis; small brown-red to orange-yellow crusts. Multiple small erosions are indicative of superficial BCC.
- Not specific for BCC -- also seen in melanoma, SCC, or traumatized lesions.
Shiny white blotches and strands (polarized light only):
- Blotches: white homogeneous clods. Strands: parallel, linear white areas that are longer than shiny white lines and do not intersect orthogonally.
- Combined presence is highly specific for BCC.
- Histologically: strands correspond to stromal alteration; blotches to stromal alteration around BCC tumor islands or collections of mucin.
Multiple aggregated yellowish-whitish globules (MAY globules):
- Clustered yellow-white globules visible with both polarized and nonpolarized light.
- Strongly associated with BCC (also seen in desmoplastic trichoepitheliomas).
- Negatively associated with superficial BCC; positively associated with deeper, higher-grade subtypes.
- Histologically: calcifications and keratocysts.
Arborizing vessels:
- Bright red, large-diameter vessels with distinct treelike branching into more delicate capillaries; appear sharply in-focus.
- Highly suggestive of nodular BCC (also seen in melanoma, hypertrophic scars/keloids, epidermal cysts, AK, intradermal nevi).
- Histologically (in BCC): neovascular vessels surrounding BCC tumor aggregates in the dermis.
BCC subtype prediction by dermoscopy:
| Dermoscopic Features | BCC Subtype |
|---|---|
| Multiple small erosions, flat surface, leaf-like structures, atypical vessels | Superficial BCC |
| Arborizing vessels, blue ovoid nests, ulceration, MAY globules | Nonsuperficial (mostly nodular) BCC |
4.4.2 Keratinizing Tumors (AK, SCC, Keratoacanthoma)
White circles:
- Bright white circles surrounding yellow/orange keratin plugs.
- Histologically: acanthosis and hypergranulosis of the infundibular epidermis.
- Highly suggestive of well-differentiated SCC and keratoacanthoma.
Dark dots/globules or circles in a linear arrangement:
- Brown dots/globules arranged linearly.
- Frequently found in pigmented SCC in situ (Bowen disease).
- Histologically: aggregates of atypical basal pigmented keratinocytes.
- Small brown circles in pigmented Bowen disease: pigmented basal keratinocytes + foci of undulated DEJ.
Strawberry pattern:
- Reddish pseudonetwork interrupted by prominent follicular openings.
- Histologically: localized increase in cutaneous vasculature surrounding dilated adnexal openings filled with keratin.
- Highly suggestive of nonpigmented actinic keratosis (AK).
Rosettes (see Section 4.2.10): Common in actinically damaged skin, AK, and SCC.
Scale:
- Homogeneous opaque yellow/brown structures.
- Histologically: hyperkeratosis and parakeratosis.
- Commonly seen in AK, SCC, and inflammatory dermatoses.
Inner gray halo:
- Grayish hue on the inner side of the follicular opening.
- Associated with pigmented AK.
- Histologically: hypergranulosis with pigmentation of basal keratinocytes of the infundibular opening.
- Not to be confused with circle-within-circle or gray follicular openings in melanoma.
SCC subtype prediction by dermoscopy:
| Dermoscopic Features | SCC Subtype |
|---|---|
| Glomerular vessels | Bowen disease |
| Dark dots/globules/circles linearly arranged | Pigmented Bowen disease |
| Strawberry pattern | Actinic keratosis |
| Bleeding; vessels in >50% of tumor surface, diffuse arrangement | Poorly differentiated SCC |
| Looped vessels, white circles | Well-differentiated SCC |
4.4.3 Seborrheic Keratoses (SK)
Fissures and ridges (formerly sulci and gyri):
- Fissures: invaginations of the epidermis. Ridges: raised portions of the epidermis.
- Create a "brain-like" appearance.
- Histologically: thickened epidermis with epidermal clefts filled with keratin.
Milia-like cysts:
- Shiny whitish to yellowish round structures; more conspicuous with nonpolarized dermoscopy.
- Histologically: intraepidermal keratin pseudocysts.
- Multiple milia-like cysts are highly suggestive of SK. Isolated ones can also be seen in BCC, congenital nevi, papillomatous melanocytic nevi, and even melanoma.
Comedo-like openings and crypts:
- Comedo-like openings: dark brown/black round to oval invaginations. Crypts: more elongated versions.
- Histologically: epidermal invaginations filled with keratin.
- Multiple comedo-like openings are associated with SKs but can also be seen in any papillomatous lesion (intradermal nevi, melanoma).
4.4.4 Angioma and Angiokeratoma
Lacunae:
- Multiple well-demarcated round to oval reddish structures arranged in clusters, separated by whitish rims (septae).
- Histologically: dilated, thin-walled vessels in the papillary dermis.
- Hallmark of vascular tumors (mainly angiomas).
Dark/thrombosed lacunae (violaceous, blue-black, or black):
- Seen in thrombosed angiomas and angiokeratomas.
- Histologically: partially or completely thrombosed dermal vessels.
Targetoid hemosiderotic angiokeratoma:
- Central dark lacuna surrounded by peripheral red-brownish homogeneous area.
- Histologically: less dilated angulated vascular spaces, hemosiderin deposition, and extravasated erythrocytes in the mid and deep dermis.
4.4.5 Dermatofibroma
Central white patch:
- White structureless area located centrally, surrounded by a thin tan network.
- Histologically: fibrosis in the papillary dermis.
- Highly suggestive of dermatofibroma when combined with a delicate peripheral network.
Peripheral delicate network:
- Thin brown lines forming a meshwork pattern at the periphery.
- Histologically: hyperpigmentation of basal keratinocytes.
Ring-like globules:
- The peripheral network can transition from thin lines at the periphery to larger donut-shaped ringed globular structures toward the central scarlike area.
- Histologically: broadened rete ridges associated with dermatofibromas.
4.4.6 Lichen Planus-Like Keratosis (LPLK)
LPLK is an inflammatory process occurring when a solar lentigo or SK undergoes involution/regression.
Diffuse gray dots:
- Most prevalent finding in LPLK.
- Histologically: melanophages in the papillary dermis, corresponding to the final stages of the LPLK regression process.
Additional LPLK patterns and their histologic correlates:
| Pattern | Histologic Correlate | Stage |
|---|---|---|
| Pinkish areas | Capillary dilatation and lichenoid inflammation | Inflammatory stage |
| Annular/granular pattern | Melanophages surrounding hair follicles | Regression stage |
| Gray pseudonetwork | Aggregates of melanophages in the papillary dermis | Regression stage |
| Shiny white structures | Stromal alteration | Regression stage |
Clinical Scenario
A 52-year-old woman presents with a pearly, slightly translucent papule on the nose that has been present for 8 months. Dermoscopy with polarized light reveals bright red, sharply focused vessels with distinct treelike branching (arborizing vessels), several well-circumscribed blue-gray oval structures, and white linear parallel structures (shiny white blotches and strands). No pigment network is present.
What is your diagnosis and key dermoscopic findings?
Pigmented basal cell carcinoma (nodular subtype)
The arborizing vessels correspond histopathologically to neovascular vessels surrounding BCC tumor aggregates in the dermis, and are highly suggestive of nodular BCC. The blue-gray ovoid nests represent large pigmented BCC tumor nodules in the dermis. The shiny white blotches and strands (visible only with polarized light) correspond to stromal alteration around BCC tumor islands and collections of mucin, and their combined presence is highly specific for BCC. The absence of pigment network helps exclude melanocytic origin.
4.4.7 Clear Cell Acanthoma
Vessels in a string of pearls arrangement:
- Dotted or glomerular vessels following a serpiginous arrangement.
- Histologically: dilated vessels filling the tips of dermal papillae.
4.4.8 Sebaceous Neoplasms
Crown vessels:
- Radial, serpentine, or arborizing vessels at the periphery of the lesion that radiate toward the center but do not cross the midline.
- Histologically: dermal vessels displaced by aggregated lobules of hyperplastic sebaceous glands.
- Associated with sebaceous hyperplasia, nevus sebaceous, and sebaceous adenoma.
"Popcorn-like structures" (cloud structures):
- Polylobular yellowish to whitish structures.
- Commonly found in sebaceous neoplasms.
- Histologically: hypertrophied dermal sebaceous glands.
4.4.9 Porokeratosis
Peripheral annular double-rim ("white track"):
- Well-defined, thin white-yellow annular structure surrounding a pink to whitish central flat area. Often slightly raised with rough texture.
- Histologically: cornoid lamella (the pathognomonic histologic feature of porokeratosis).
Check Your Understanding
What dermoscopic structure corresponds to the large dilated vessels in basal cell carcinoma, and why are they arborizing?
Arborizing vessels in BCC correspond to thickened, dilated blood vessels in the dermis. They branch dichotomously because BCC tumor islands displace and compress surrounding stroma, causing vessels to grow in a tree-like branching pattern around the tumor lobules.
Key Takeaways
- Leaf-like areas and spoke-wheel structures are diagnostic of pigmented BCC, corresponding to basaloid nests at the DEJ.
- Arborizing vessels (bright red, sharply focused, branching) correlate with dilated arterioles feeding the BCC tumor and are best seen with polarized dermoscopy.
- Comedo-like openings and milia-like cysts are hallmarks of seborrheic keratosis, corresponding to keratin-filled invaginations and intraepidermal horn cysts respectively.
4.5 Inflammoscopy Correlates
Inflammoscopy is the dermoscopic evaluation of inflammatory dermatoses.
4.5.1 Psoriasis
Monomorphic red dots with white scales:
- Monomorphic and symmetrically distributed red dots over an erythematous background, together with white adherent scales.
- This is the hallmark pattern of psoriasis.
- Histologically: spiraled capillaries in the papillary dermis, psoriasiform epidermal hyperplasia, and parakeratosis.
4.5.2 Dermatitis
Irregularly distributed red dots with yellow scales/crusts:
- The most frequent dermoscopic features of dermatitis (allergic/contact, atopic, seborrheic).
- Yellow crusts/scales are frequent in acute stages.
- Histologically: irregular red dots correspond to slight dilatation of subpapillary vessels; yellow crusts/scale correspond to the epidermal spongiotic reaction.
4.5.3 Lichen Planus
Peripheral dotted/linear vessels with whitish structures (Wickham striae):
- Peripheral dotted or linear vessels together with round, linear, reticular, or annular pearly-whitish structures.
- Histologically: the whitish structures correspond to compact orthokeratosis above zones of wedge-shaped hypergranulosis and acanthosis. This is the dermoscopic equivalent of Wickham striae.
4.5.4 Rosacea
Polygonal vessels:
- Linear vessels arranged in horizontal and vertical lines forming a geometrical pattern.
- In the absence of scale, highly specific for erythemato-telangiectatic rosacea.
- Histologically: intense vasodilatation.
4.5.5 Granulomatous Skin Diseases
Orange-yellowish patches:
- Round to oval orange-yellowish patches/plaques.
- Characteristic of many granulomatous cutaneous disorders: leishmaniasis, sarcoidosis, lupus vulgaris, granuloma faciale, granulomatous rosacea, granuloma annulare.
- Histologically: granulomas located superficially in the dermis.
4.6 Infectious Disease Correlates
4.6.1 Molluscum Contagiosum
White/yellow amorphous structures with "red corona":
- Polylobular whitish to yellowish structures surrounding a central indentation or dell.
- Linear or branched vessels ("red corona" or crown vessels) at the periphery.
- Histologically: endophytic lobules of hyperplastic squamous epithelium expanding into the dermis, displacing dermal dilated vessels.
- Note: Can mimic sebaceous hyperplasia dermoscopically.
4.6.2 Warts
Multiple dark dots:
- Black/red dots within a well-defined yellowish area.
- Characteristic of plantar warts.
- Histologically: a recent study of palmoplantar warts found no thrombosed vessels, suggesting that the dark dots are secondary to intracorneal hemorrhages rather than dermal microthrombi.
4.6.3 Scabies
Dark brown triangular structures ("delta-wing jet sign"):
- Small brown triangular structure located at the end of a whitish curved line.
- Dermoscopic sensitivity for scabies can be as high as 0.91 (higher than skin scraping); specificity approximately 0.46.
- Histologically: the brown triangle corresponds to the pigmented anterior part of the scabies mite (Sarcoptes scabiei). The whitish curved line corresponds to the burrow of the mite.
Check Your Understanding
What dermoscopic finding is characteristic of scabies, and what does it correspond to histologically?
The jet-with-contrail sign is characteristic of scabies. The dark triangular structure at the leading edge corresponds to the mite itself (including its pigmented anterior portion), while the trailing white-to-brown line corresponds to the burrow (tunnel) in the stratum corneum.
4.7 Trichoscopy Correlates
Trichoscopy is the dermoscopic study of inflammatory, infectious, and artefactual hair and scalp disorders.
4.7.1 Yellow Dots
- Appearance: Round yellowish to pinkish structures.
- Histopathologic correlate: Distended follicular infundibulum plugged with keratin and sebum.
- Associated disorders: Characteristic of alopecia areata (AA); also seen in androgenetic alopecia and other scalp disorders.
4.7.2 Black Dots
- Appearance: Round dark structures inside the follicular ostia ("cadaverized hairs").
- Histopathologic correlate: Stubs of hairs fractured before their emergence from the scalp.
- Associated disorders: Alopecia areata (sign of disease activity).
4.7.3 Pinpoint White Dots
- Appearance: Small round whitish structures.
- Histopathologic correlate: Follicular and sweat gland openings.
- Associated disorders: Seen in healthy scalp and all types of alopecia (nonspecific finding).
4.7.4 White Patches
- Appearance: Large and irregular pale structures.
- Histopathologic correlate: Destroyed follicles replaced by fibrous tracts and focal absence of melanin (dermal fibrosis).
- Associated disorders: Cicatricial (scarring) alopecias such as frontal fibrosing alopecia.
4.7.5 Blue-Gray Dots
- Appearance: Round grayish structures.
- Histopathologic correlate: Melanophages in the dermis.
- Two patterns:
- Target pattern: Melanin around the hair follicle; pigmentary incontinence restricted to follicular units. Seen in lichen planopilaris (LPP).
- Speckled pattern: Melanin in interfollicular areas. Seen in discoid lupus erythematosus.
4.7.6 Empty Follicles
- Appearance: Skin-colored small depressions without hairs.
- Histopathologic correlate: Empty infundibula.
- Associated disorders: Alopecia areata, telogen effluvium, androgenetic alopecia.
4.7.7 Absence of Follicular Openings
- Appearance: Dermoscopy demonstrates a complete lack of hair follicles.
- Histopathologic correlate: Dermal fibrosis.
- Associated disorders: Characteristic of scarring (cicatricial) alopecia.
4.7.8 Peripilar Casts
- Appearance: Concentrically arranged scales surrounding the hair shaft.
- Histopathologic correlate: Perifollicular inflammation.
- Associated disorders: Frequently seen in lichen planopilaris (LPP); also in other scarring alopecias and keratinization disorders.
4.7.9 Peripilar Sign
- Appearance: Brown halo surrounding the follicular ostium.
- Histopathologic correlate: Perifollicular inflammation.
- Associated disorders: Often seen in androgenetic alopecia.
4.7.10 Follicular Keratotic Plugging
- Appearance: Yellow-brownish round structures larger than dots.
- Histopathologic correlate: Hyperkeratosis and keratin material occluding dilated infundibular openings.
- Associated disorders: Discoid lupus erythematosus.
4.7.11 Additional Trichoscopy Features
Red dots (trichoscopy):
- Round red structures regularly distributed around follicular openings.
- Histologically: widened follicular ostia surrounded by dilated vessels.
- Associated with discoid lupus erythematosus.
Pigment pattern / honeycomb pattern:
- Meshwork composed of brown lines and holes on the scalp.
- Histologically: lines correspond to pigmented rete ridges.
- Associated with ultraviolet exposure.
5. Dermoscopic Structure-Histology Reference Table
5.1 Melanocytic Neoplasms
| Dermoscopic Structure | Descriptive Term | Histopathologic Correlate |
|---|---|---|
| Pigmented network (typical) | Lines, reticular | Melanin in keratinocytes/melanocytes along regular rete ridges; holes = suprapapillary plates |
| Pigmented network (atypical) | Lines, reticular, irregular | Disarranged rete ridges; confluent melanocytic nests; irregular melanin distribution |
| Negative pigment network | Lines, reticular, hypopigmented, around brown clods | Broadened rete ridges with hypergranulosis surrounding junctional melanocyte proliferation; bridging of rete ridges |
| Angulated lines | Lines, angulated or polygonal | Atypical melanocytes and melanophages at the basal layer; flat DEJ with pagetoid spread |
| Globules (brown/black) | Clods, round or oval | Melanocytic nests at the DEJ or epidermis |
| Globules (blue) | Clods, blue | Melanocytic nests in the dermis |
| Globules (white) | Clods, white | Balloon cell changes in melanocytes |
| Dots (black) | Dots, black | Melanin in upper epidermis / stratum corneum |
| Dots (brown) | Dots, brown | Small melanocytic nests at epidermis or DEJ |
| Dots (blue-gray) | Dots, gray | Melanin in upper dermis or dermal melanophages |
| Dots (red) | Dots, red | Vessels in dermis |
| Streaks / pseudopods | Lines, radial, at periphery | Linearly confluent junctional nests of pigmented melanocytes at lesion periphery |
| Homogeneous blue pattern | Structureless blue | Dense pigmented melanocytes or melanophages in dermis |
| Blotches | Structureless zone, brown or black | Abundant melanin in one or more epidermal layers +/- dermis |
| Black lamella | Structureless dark, superficial | Excessive melanin in stratum corneum (tape-strippable) |
| Granularity / peppering | Dots, gray, multiple | Free melanin or melanophages in dermis (regression) |
| Scarlike depigmentation | Structureless zone, white | Dermal fibrosis |
| Shiny white lines | Lines, white, perpendicular (polarized only) | Birefringent collagen bundles (altered/new collagen) |
| Blue-whitish veil | Structureless zone, blue + white haze | Heavily pigmented dermal melanocytes + acanthosis + compact orthokeratosis |
5.2 Special Sites
| Site | Dermoscopic Structure | Histopathologic Correlate |
|---|---|---|
| Face | Pseudonetwork | Pigmented cells in epidermis with flat DEJ interrupted by follicular openings |
| Face (LM) | Gray dots (perifollicular) | Free melanin/melanophages in dermis around follicles |
| Face (LM) | Concentric circles | Increased melanocytes in follicular epithelium + surrounding rete ridge |
| Face (LM) | Angulated lines / rhomboids | Flat DEJ + pagetoid spread + melanophages |
| Volar | Parallel furrow pattern | Melanocytes in crista limitans (furrows) |
| Volar | Parallel ridge pattern | Melanocyte proliferation around acrosyringia (crista profunda intermedia) |
| Volar | Lattice-like pattern | Anatomical variant of furrow pattern |
| Volar | Fibrillar pattern | Melanin columns angled by mechanical forces in thick stratum corneum |
| Mucosa | Homogeneous pattern | Flattened rete ridges with acanthosis |
| Mucosa | Ring-like / fish scale pattern | Hyperpigmented widened rete ridges skipping narrow dermal papillae |
| Mucosa | Parallel / hyphal pattern | Hyperpigmentation at tips of obliquely elongated rete |
| Mucosa | Dotted-globular pattern | Aggregated melanin in upper lamina propria |
| Nails | Regular gray band | Basal layer pigmentation (activation), no melanocyte hyperplasia |
| Nails | Regular brown band | Benign melanocytic hyperplasia, no nests |
| Nails | Irregular band (multiple colors, variable thickness) | Disorganized atypical melanocyte proliferation (melanoma) |
5.3 Nonmelanocytic Neoplasms
| Dermoscopic Structure | Tumor Type | Histopathologic Correlate |
|---|---|---|
| Leaf-like areas | BCC | Pigmented BCC nests at DEJ and papillary dermis |
| Spoke wheel areas | BCC | Pigmented BCC nests/cords at DEJ and upper dermis |
| Concentric globular structures | BCC | Same as spoke wheel areas |
| Blue-gray ovoid nests | BCC | Large pigmented BCC tumor nodules in dermis |
| Blue-gray globules | BCC | Pigmented BCC aggregates in dermis |
| Blue-gray dots (buckshot) | BCC | Small BCC aggregates at DEJ / papillary dermis |
| Arborizing vessels | BCC | Neovascular vessels surrounding BCC tumor aggregates |
| Shiny white blotches and strands | BCC | Stromal alteration; mucin collections |
| MAY globules | BCC | Calcifications and keratocysts |
| Ulceration | BCC (nodular) | Loss of entire epidermis |
| Multiple small erosions | BCC (superficial) | Partial epidermal loss |
| White circles | SCC / keratoacanthoma | Acanthosis + hypergranulosis of infundibular epidermis |
| Dots/globules linearly arranged | Pigmented Bowen disease | Atypical basal pigmented keratinocytes |
| Strawberry pattern | Actinic keratosis | Increased vasculature around dilated keratin-filled adnexal openings |
| Inner gray halo | Pigmented AK | Hypergranulosis + pigmented basal keratinocytes at infundibulum |
| Rosettes | AK, SCC | Hyperkeratosis in follicular openings; perifollicular fibrosis |
| Scale | AK, SCC | Hyperkeratosis and parakeratosis |
| Fissures and ridges | SK | Thickened epidermis with keratin-filled epidermal clefts |
| Milia-like cysts | SK | Intraepidermal keratin pseudocysts |
| Comedo-like openings / crypts | SK | Epidermal invaginations filled with keratin |
| Lacunae (red) | Angioma | Dilated, thin-walled vessels in papillary dermis |
| Lacunae (dark/thrombosed) | Angiokeratoma | Partially or completely thrombosed dermal vessels |
| Central white patch | Dermatofibroma | Fibrosis in papillary dermis |
| Delicate peripheral network | Dermatofibroma | Hyperpigmented basal keratinocytes |
| Diffuse gray dots | LPLK | Melanophages in papillary dermis (regression) |
| String of pearls vessels | Clear cell acanthoma | Dilated vessels in tips of dermal papillae |
| Crown vessels | Sebaceous neoplasms | Dermal vessels displaced by hyperplastic sebaceous lobules |
| Popcorn-like structures | Sebaceous neoplasms | Hypertrophied dermal sebaceous glands |
| Peripheral annular double-rim | Porokeratosis | Cornoid lamella |
5.4 Inflammatory and Infectious Conditions
| Dermoscopic Finding | Condition | Histopathologic Correlate |
|---|---|---|
| Monomorphic red dots + white scales | Psoriasis | Spiraled papillary capillaries + psoriasiform hyperplasia + parakeratosis |
| Irregular red dots + yellow scales | Dermatitis | Dilated subpapillary vessels + epidermal spongiosis |
| Whitish structures (Wickham striae) + dotted/linear vessels | Lichen planus | Compact orthokeratosis + wedge-shaped hypergranulosis + acanthosis |
| Polygonal vessels (no scale) | Rosacea | Intense vasodilatation |
| Orange-yellowish patches | Granulomatous diseases | Superficial dermal granulomas |
| White/yellow amorphous structures + red corona | Molluscum contagiosum | Endophytic hyperplastic squamous lobules + displaced dilated vessels |
| Multiple dark dots in yellowish area | Warts | Intracorneal hemorrhages |
| Brown triangular structure + whitish curved line | Scabies | Pigmented anterior part of mite + mite burrow |
5.5 Trichoscopy
| Trichoscopic Structure | Histopathologic Correlate | Associated Disorder(s) |
|---|---|---|
| Yellow dots | Distended infundibulum with keratin + sebum | Alopecia areata, androgenetic alopecia |
| Black dots ("cadaverized hairs") | Hair stubs fractured before scalp emergence | Alopecia areata (active) |
| Pinpoint white dots | Follicular and sweat gland openings | Normal scalp, all alopecias |
| White patches | Destroyed follicles replaced by fibrous tracts; focal melanin absence | Cicatricial alopecia |
| Blue-gray dots (target pattern) | Perifollicular melanophages | Lichen planopilaris |
| Blue-gray dots (speckled pattern) | Interfollicular melanophages | Discoid lupus erythematosus |
| Empty follicles | Empty infundibula | AA, androgenetic alopecia, telogen effluvium |
| Absence of follicular openings | Dermal fibrosis | Scarring alopecia |
| Peripilar casts | Perifollicular inflammation | LPP, frontal fibrosing alopecia |
| Peripilar sign (brown halo) | Perifollicular inflammation | Androgenetic alopecia |
| Follicular keratotic plugging | Hyperkeratosis occluding dilated infundibula | Discoid lupus erythematosus |
| Red dots (around follicles) | Widened ostia + dilated vessels | Discoid lupus erythematosus |
6. Clinical Pearls
Color = Depth rule: In melanocytic lesions, dermoscopic color is a proxy for melanin depth. Black = stratum corneum/upper epidermis; brown = DEJ; gray = papillary dermis; blue = deeper dermis. Master this relationship and you can estimate the histologic level of pigment from dermoscopy alone.
Tape-stripping for black lamellae: If a lesion shows a suspicious-looking off-center blotch, consider that it may be a black lamella (melanin in the stratum corneum). Tape-stripping the stratum corneum can reveal the underlying benign network, potentially avoiding an unnecessary biopsy. The black lamella reappears in 3-12 months.
Negative network vs. shiny white lines: Both can create grid-like patterns, but negative network is visible with both polarized and nonpolarized light, while shiny white lines appear only under polarized light and display angular dependence (conspicuity changes with rotation of the dermatoscope). They commonly coexist in melanoma and Spitz nevi.
Symmetry of streaks matters: Symmetrical distribution of streaks around the entire periphery favors Reed's nevus. Asymmetrical or focal peripheral streaks favor superficial spreading melanoma. This single observation can make the difference between reassurance and biopsy.
BAP1-inactivated melanocytic tumor clue: A focal eccentric cluster of globules at the periphery of a raised, otherwise homogeneous melanocytic lesion should raise suspicion for a BIMT ("bapoma"). If multiple such lesions are present, consider screening for the BAP1 tumor predisposition syndrome (uveal melanoma, mesothelioma, renal cell carcinoma risk).
Parallel ridge = biopsy: On volar skin, the parallel ridge pattern (pigment on the ridges) is the most reliable dermoscopic indicator of acral melanoma. The parallel furrow pattern (pigment in the furrows) is associated with benign nevi. When in doubt, applying the dermatoscope at an angle can help distinguish fibrillar patterns arising from furrows vs. ridges.
BWV location tells the story: The blue-whitish veil corresponds to palpable/raised areas of a melanoma. If you see BWV in an SK, look carefully for comedo-like openings and milia-like cysts within it -- their presence helps confirm SK rather than melanoma.
Ulceration in untreated BCC predicts treatment response: The presence of ulceration in a nontreated BCC has been associated with an excellent response to imiquimod.
Polarized-only structures: Remember that shiny white structures (lines, blotches/strands, rosettes) can only be seen with polarized dermoscopy. Always examine suspicious lesions with both polarized and nonpolarized light, as each modality reveals different information.
Dermoscopy predicts melanoma genetics: Certain dermoscopic patterns correlate with specific mutations -- dotted vessels with BRAF wild-type; ulceration, BWV, and irregular peripheral streaks with BRAF mutations; peppering/granularity with BRAF/NRAS mutations; dark homogeneous streaks with KIT mutations.
Micro-Hutchinson's sign -- proceed with caution: While this is an important clue for nail apparatus melanoma, a negative cuticle biopsy does not exclude melanoma in the matrix. The biopsy must sample the matrix itself to be definitive.
Inflammoscopy differentiation: Psoriasis shows monomorphic, symmetrically distributed red dots + white scales. Dermatitis shows irregularly distributed red dots + yellow scales/crusts. This simple distinction has high clinical utility and directly reflects the underlying histopathology (psoriasiform hyperplasia vs. spongiosis).
8. Cross-References
| Topic | Pages |
|---|---|
| Introduction (dermoscopy as diagnostic bridge) | pp. 10 |
| Colors in dermoscopy (melanin depth, chromophores) | pp. 10 |
| Pigmented network | pp. 10-11 |
| Negative network | pp. 11 |
| Angulated lines | pp. 11 |
| Globules | pp. 11-13 |
| Dots | pp. 13 |
| Streaks | pp. 13 |
| Homogeneous blue pattern | pp. 13 |
| Blotches | pp. 13-15 |
| Regression structures | pp. 15 |
| Shiny white structures | pp. 15-18 |
| Blue-whitish veil | pp. 18 |
| Facial skin (pseudonetwork, LM features) | pp. 18-19 |
| Volar skin (parallel patterns) | pp. 19-22 |
| Mucosal sites | pp. 22 |
| Nails | pp. 23-24 |
| BCC (leaf-like, spoke wheel, ovoid nests, vessels, MAY globules) | pp. 24-28, Tables 3.4-3.5 |
| Keratinizing tumors (AK, SCC) | pp. 28-29 |
| Seborrheic keratoses | pp. 29 |
| Angioma and angiokeratoma | pp. 29 |
| Dermatofibroma | pp. 29-30 |
| LPLK | pp. 30 |
| Clear cell acanthoma | pp. 30 |
| Sebaceous neoplasms | pp. 30-31 |
| Porokeratosis | pp. 31 |
| Inflammoscopy (psoriasis, dermatitis, lichen planus, rosacea, granulomatous) | pp. 31-32 |
| Infectious diseases (molluscum, warts, scabies) | pp. 32-34 |
| Trichoscopy | pp. 34-35 |
| Diagnostic improvement and ex vivo dermoscopy | pp. 35-36 |
| Prognostic predictions (melanoma) | pp. 36 |
| BCC subtype prediction | pp. 36 |
| SCC subtype prediction | pp. 36 |
| Genetic correlations (melanoma) | pp. 37 |
| Key points | pp. 37 |
9. Related Modules
Prerequisite
- Module 01: Introduction & Principles of Dermoscopy -- foundational knowledge of dermoscope types (polarized vs. nonpolarized), contact vs. noncontact dermoscopy, and image capture techniques is essential background for understanding histopathologic correlations.
Modules That Build on This Content
- Module 03: Pattern Analysis Revised -- applies the structures described here as building blocks for pattern analysis.
- Module 04: Top-Down 2-Step Algorithm -- uses structure recognition for step 1 (benign recognition) and step 2 (equivocal lesion analysis).
- Module 05: Prediction without Pigment -- extends concepts of vascular patterns and shiny white structures to nonpigmented lesions.
- Module 06: Chaos and Clues Triage Algorithm -- the 8 clues to malignancy are largely based on the structures and their histopathologic correlates covered in this module.
- Module 07: TADA and Other Triage Algorithms -- uses dermoscopic features described here as input criteria for multiple scoring systems.
Deeper Explorations of Specific Topics
- Module 09: Basal Cell Carcinoma -- detailed BCC dermoscopy including all structures introduced in Section 4.4.1.
- Module 10: Actinic Keratosis -- expanded coverage of the strawberry pattern, rosettes, and AK-specific features.
- Module 11: SCC Spectrum -- deeper exploration of keratinizing tumor dermoscopy.
- Module 12: Solar Lentigines, SK, and LPLK -- expanded coverage of SK features and LPLK regression patterns.
- Module 13: Vascular Lesions -- comprehensive coverage of lacunae and vascular dermoscopy.
- Module 19: Spitz and Reed Nevi -- detailed coverage of streaks, negative network, and starburst pattern.
- Module 23: Lentigo Maligna -- full progression model of LM dermoscopy on facial skin.
- Module 24: Acrolentiginous Melanoma -- expanded coverage of parallel ridge and furrow patterns.
- Module 30: Face -- comprehensive facial dermoscopy with pseudonetwork and facial algorithms.
- Module 31: Palms and Soles -- detailed volar skin dermoscopy.
- Module 32: Mucosal Surfaces -- mucosal dermoscopy patterns and melanoma clues.
- Module 33: Nails -- nail apparatus dermoscopy and melanonychia algorithm.
- Module 34: Hair and Scalp (Trichoscopy) -- comprehensive trichoscopy coverage.
- Module 35: Dermoscopy in Infectious Diseases -- expanded coverage of molluscum, warts, scabies.
- Module 36: Inflammoscopy -- comprehensive inflammatory dermatosis dermoscopy.
Module 02 -- Version 1.0 Part of the Dermoscopy Educational Course.
Image Sources & Citations
- DERM12345 (Skin Lesion Dataset with 40 Subclasses): DERM12345: A Large-scale Skin Lesion Image Dataset with 40 Subclasses. Figshare. 2023. License: CC-BY-4.0.
- HIBA Dermoscopy Dataset: HIBA Dermoscopy Dataset. Hospital Italiano de Buenos Aires. License: CC-BY-4.0.